How the LM causes GE reflux
![]()
Introduction
Gastro-esophageal reflux (GER) is the preeminent esophageal disorder. It causes
or accompanies most other esophageal problems, making a major contribution to
the sum of human misery. In the United States alone, the provision of over-the-counter
antiacid remedies was a $700 million to $800 million a year industry(1)
in 1985 with sales exceeding even the $556,000,000 annual expenditures for cold
remedies.(2) Cimetidine has passed Valium as
number one in the marketplace.(3) About eight
billion times a year, someone in the US is sufficiently distressed to take a
Tum, Rolaid or Alka-Seltzer - a staggering statistic that does not even include
the (forbidden) usage of bicarbonate of soda.
Although current opinion(4) leans toward the
view that reflux is primarily due to hypotension of the LES,(5)
I will show that reflux is an effect of LMC. Because an open sphincter will
result in reflux, the next proposition to be proved is this:
LM contraction (LMC) is the efficient cause of reflux.
The force produced by longitudinal muscle contraction is resolved by the phrenoesophageal
ligament (PEL) into two components: one component stretches the PEL, causing
"hiatus hernia"; the other opens the sphincter, causing reflux.
The angle of His and the subdiaphragmatic esophageal segment, structures that
form the theoretical underpinnings of surgical intervention, prove to be nonexistent.
Once the lower esophageal sphincter is recognized as the sole defense against
reflux, a wealth of clinical, surgical and radiological phenomena to be cited
will show that this thesis is correct.
The clinical background of reflux
Several inciting factors are known to cause reflux. The most familiar are dietary
indiscretions. Of the various foods that promote heartburn, many fall into a
class of essential oils known as carminatives, nearly all of which lower LES
pressure (LESP). Included are onions, garlic, peppermint, spearmint, cinnamon,
dill, fennel, ginger, rosemary, caraway and cloves.(6)
Onions are the most common offenders. There are people, particularly those who
dine in restaurants, who have a great tolerance for onions and can eat them
with impunity. To pyrosis sufferers on the contrary, they are poison. Because
heartburn is delayed in onset, one cannot say that direct irritation of the
esophagus is responsible. Either time is required for the active principal to
take effect, partial digestion releases the inciting factor or a still more
indirect action relates cause with effect.
Virtually every food that can cause an "upset stomach" is an inciting agent
for heartburn - Tabasco sauce, hot peppers, Italian dressing, barbecue sauce,
nutmeg, chocolate, smoky links, alcohol, histamine, fatty foods. It is significant
that the "gas" producing foods - especially cucumbers and members of the cabbage
family are on the list.
These and other substances known to provoke reflux are generally either stimulants
or irritants. It would be more in keeping with the normal physiological pattern
if the provocative agent stimulated an end organ than inhibited the sphincter.
One searches in vain for an example of an irritant or stimulant that relaxes.
All one can say with certainty is that there is an active principal that,
introduced into the alimentary tract of susceptible individuals, will cause
reflux of gastric contents into the esophagus.
Smoking (nicotine?) and coffee are inciting agents. Pregnancy has a long term provocative effect now considered due to endogenous progesterone. Birth control preparations may have the same effect due to exogenous progesterone.
The intermittent nature of reflux, its provocation by foods or drugs, and its
consistency in a given individual set the parameters within which the search
for a solution of the reflux problem should be conducted. Anatomy is constant;
reflux is intermittent. Clearly, this shows that reflux is a physiological,
not an anatomical problem. In some fashion, reflux must be tied to the chemical
nature of the provocative agents. Strangely, the search for the cause and cure
of reflux has focused on illusory anatomical structures.
Conventional theories of the antireflux mechanism
Of the proposed mechanisms for the prevention of reflux, only three have survived. The physiologic sphincter - that dominates the interest of basic researchers and clinical esophageal physiologists - the "subphrenic esophageal segment" and the slightly acute angle (of His) between the esophagus and the fundus shown in anatomy books. Because it still influences surgical treatment (Nissen fundoplication, Belsey Mark IV, Hill, and others), the latter must be considered in detail.
![]()
The angle of His
Johnstone(7) has suggested that the idea that
the angle of His prevented reflux may have been founded on the clinical observation
that reflux is rare in "paraesophageal" HH's - a type of HH with an acute angle
of His.
We pay lip-service to the truism that living anatomy differs from that seen
in the cadaver, but often not where it counts. The angle of His, if it existed,
should be seen in normal patients on upper GI examination. It is not. Yet highly
competent surgeons design anti-reflux operations to create this artifact.
Why is the angle of His seen in the cadaver and in the anesthetized surgical
patient but not in the living, awake subject? Because in the dead or anesthetized
the LM is atonic. In the living subject, the basal tone of the LM pulls the
fundus up against the diaphragm, obliterating the angle seen in the cadaver
or at laparotomy. When a surgeon applies traction to the lesser curvature of
the stomach to visualize the hiatal area, he creates the angle by opposing LM
traction. For much the same reasons - the LM expires with the patient or is
overcome by traction and anesthesia - anatomists and surgeons have the impression
that there is a subphrenic esophageal segment.
An angle of His is seen radiologically in abnormal situations when
the LM tone is reduced or destroyed. If a patient who has had a pulldown procedure
is reexamined before his hospital discharge, the trauma of operative stretching
will have produced an angle of His that may persist for a week or more. It soon
vanishes when LM tone returns. If the esophagus is paralyzed with anticholinergic
drugs, it becomes flaccid and an angle of His may appear. When the esophagus
recovers from the drug or the trauma, the angle vanishes.
An angle of His of an exaggerated type occurs in some cases of "paraesophageal"
hiatus hernia. Here LMC cannot snug the fundus against the diaphragm because
the fundus is above the diaphragm. With the stomach in the chest an esophagus
of normal tone and length cannot take up the slack created by loss of its inferior
attachment. Either an angle of His or a molar tooth shape results, the former
if the esophagus slides by the fundus (it is sometimes called a "rolling hiatus
hernia") the latter if it telescopes into it.
Radiologically, the only conclusion that can be drawn from an angle of His
is that the esophagus is flaccid or a HH is present. These, however, are pathologic
states. Paradoxically, we rely on a pathologic anatomical configuration
caused by death, ligamentous rupture, surgical trauma or drugs to explain the
normal competence of the cardia.
Yet, oddly enough, there is a remarkably good correlation between GE competence
and an acute angle of His.
Patients in whom an acute angle of His has been created by fundoplication
are usually greatly relieved of their reflux problem. Behar(8)
refers to the Nissen fundoplication as ". . . the most effective antireflex
procedure." not always
If counter traction is applied to the esophagus via a "pulldown" procedure,
it relieves reflux and an creates an angle of His.
If the esophagus is inactivated with anticholinergic drugs (Banthine or Probanthine)
the LM becomes flaccid, reflux is inhibited and an angle of His can form.
Finally, as already noted, patients with huge HH's - the kind diagnosed incidentally
on chest exams - often have an acute angle of His and seldom complain of reflux.
This perfect correlation explains the confidence a surgeon might well feel in the rightness of his rationale. Explaining sphincter competence on the angle of His theory, however, is a post hoc ergo propter hoc fallacy. Reducing LM tension or its vector resolution by any means corrects reflux and, incidentally, may allow formation of an angle of His. If A and B are caused by C, it does not follow that A causes B. Both gastroesophageal reflux (GER) and obliteration of the angle of His are caused by LMC not by each other. On the contrary, if death, drugs, herniation, countertraction, trauma or anesthesia overcome the sphincter-opening force of LMC, GER is cured and the angle appears.
![]()
Other objections to the angle of His hypothesis
These logical fallacies are not the only objections to the angle of His rationale
for GE competence. Structurally, it is difficult to conceive of an esophago-fundic
angle as an effective valve capable of duplicating all of the sphincter functions,
responding to reflex control, etc. The angle should form a flap valve that obturates
the mouth of the esophagus with increased intragastric pressured. Radiographs
of the region, many of them reproduced here, easily refute this idea. Even on
a priori grounds such a valve can be excluded. Such a flap would have
to be thin, but the sling fibers of the stomach that cause it when unopposed
are not a thin band. They envelope the entire fundus.
The mechanism cannot be brought into conformity with what is known about the
sphincter from manometric studies. How is this "angle valve"(9)
integrated with the peristaltic wave? How is its action recorded manometrically?
Is there an increase in intragastric pressure preceding sphincter closure? Where
is the article, "Manometric differentiation of the LES from the Valve of Guberoff?"
Pneumoperitoneum was formerly done for the treatment of pulmonary tuberculosis
and is still encountered occasionally with perforated hollow viscera. In such
patients, as Johnstone noted,(10) the fundus
hangs suspended from its esophageal attachments. It becomes merely a larger
tubular continuation of the esophagus with an angle of nearly 180 degrees. Yet
GE reflux is not a complication of pneumoperitoneum. Splenomegaly may produce
the same configuration without causing reflux.
Again, we have recourse to Occam's razor. The angle of His concept is redundant.
Demonstrably, there is a physiologic sphincter and it is not at the angle of
His.
I have marshaled the evidence against the angle of His in some detail because,
unlike some of the other conjectured closure mechanisms, it influences treatment.
The same cannot be said for the sphincter of Lerche, the Vormagen of Arnold,
the cardiac antrum of Lushka, the gastroesophageal vestibule, the epiphrenic
bell, etc. Most of these were "hiatus hernias" that the older anatomists did
not recognize.(11)
The subdiaphragmatic esophagus
Another postulated antireflux system, the "subphrenic esophageal segment,"
is frequently invoked at least as a backup mechanism for the sphincter. There
are reasons this idea has wide credence. When seen at laparotomy, traction on
the stomach to obtain exposure pulls the anesthetized esophagus down to the
limit of its tether - the PEL - creating the impression that the esophagus ends
well below the diaphragm. The PEL is usually found to be stretched in patients
having reflux operations for the same reason the patient has reflux.
Moreover, clinicians are accustomed to viewing radiographs of the GE region
made in the RAO position. In a patient with a steeply sloping diaphragm, the
hiatus is lower than the dome of the diaphragm and to the uninitiated this gives
the appearance of a subdiaphragmatic esophagus. Radiographs are seldom made
in the lateral position to show the true relationship.
A subphrenic esophagus is in many respects similar to the angle of His: it cannot exist if there is normal esophageal tone. LM tone would shorten the esophagus and pull the "subphrenic segment" through the hiatus until brought up short by the PEL. The PEL inserts at the mucosal junction sending layers above and below the sphincter(12),(13),(14),(15) so the latter must be above the obturating membrane.(16) Any intraabdominal pressure would not be backing up the sphincter, it would be below the sphincter. The distance from the lower edge of the sphincter to the ora serrata, however, is only .5 to 2.5 cm - scarcely long enough in most patients to make any difference even if it were subdiaphragmatic. But it is not. This short segment is also above the diaphragm.(17)
Most readers will recall having seen the surgical clips used in HH repairs
on chest radiographs. Invariably, most of them are above the diaphragm
once normal LM tone returns. When a hiatal margin (the distal edge of the PEL)
is tagged with a clip at surgery, the investigators(18)
have been surprised to find that on subsequent radiographs the clip is projected
above the level of the diaphragm. Obviously, the hiatal margin is elevated
when LM tone returns postoperatively.
It is difficult to explain the confidence with which manometric identification
of a subdiaphragmatic sphincter is made(19),(20)
when under the more physiologic conditions of a fluoroscopic examination, it
is nonexistent. It must be recalled that manometric measurements have proved
misleading in the past although they were universally accepted by experts for
years. The technique is not as straightforward or as simple as might be supposed.
There are numerous ways of measuring the pressures under consideration - balloon
kymography, intracorporeal strain gages, perfused and non-perfused catheters,
transducers - and the measurements are seldom in agreement. The recorded pressure
can vary appreciably with the rate of perfusion and even with the orientation
of the sidehole. In accord with Laplace's law it also varies with the diameter
of the catheter. The perfusion itself causes swallowing making absolutely baseline
conditions unattainable.
Swallowing a sizable collection of tubes - as many as 8 and at least 3 are
recommended to average out the readings - is a stressful experience initially
and continues to be so as the apparatus is withdrawn and reinserted many times
or while the patient is in unusual or uncomfortable positions. Moreover, as
can be seen in the illustrations, the esophagus senses the presence of a foreign
body and reacts by contracting the LM which has the effect of decreasing sphincter
pressure and/or hiatal squeeze - whichever is being measured.
The physics of the situation is immensely complicated and it is very difficult,
perhaps impossible, to calibrate for and correct all possible sources of error.
The expression "in our laboratories" - often meaning "Our measurements don't
agree with anybody else's, but we are internally consistent." has been a frequent
occurrence in the literature of the subject. Finally, it seems likely that manometry
cannot as a rule differentiate hiatal squeeze from sphincter pressure. It is
likely, however, that hiatal squeeze pressure is a proxy for LMC and thus for
the LES as well.
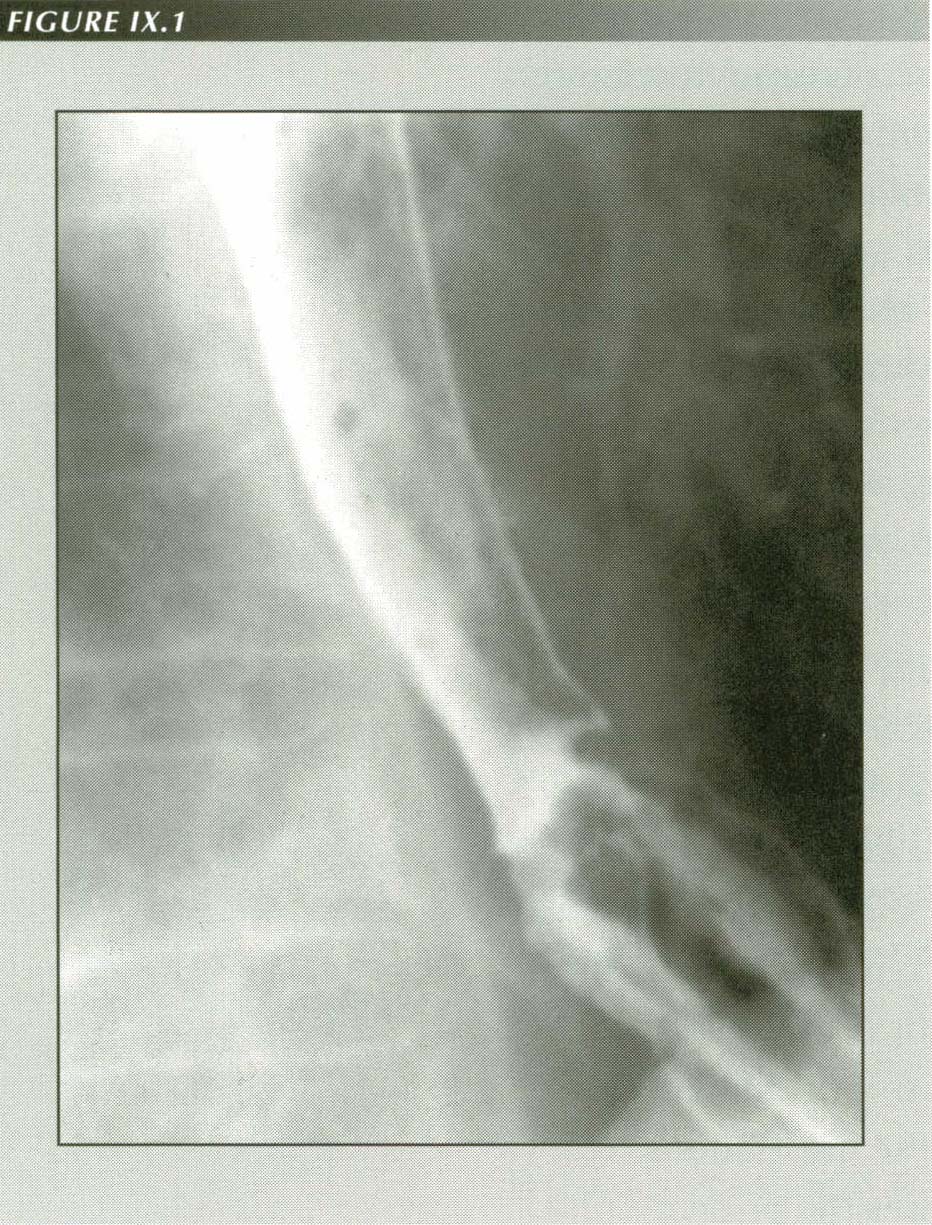
Systemic sclerosis look-alike: The circular muscle of the esophagus atrophies in systemic sclerosis while the LM is unaffected. The result is this typical appearance. the esophagus is constantly short. The HH never reduces. the sphincter never closes. As a result, there is a constant air which can be seen even on chest films. The superior constrictor does not relax which, at least in the upright position, prevents gastric fluids contacting the esophagus. There is no peristalsis below the striated muscle portion. Note the relatively small hiatus and turgid gastric mucosal in the transtracted stomach. The patient is a 71 year old undifferentiated schizophrenic on long-term haloperidol (Haldol) medication. He also had megaduodenum and pseudo-intestinal obstruction but did not exhibit Renaund�s phenomenon. Such drugs may mimic systemic sclerosis.
However, as with the angle of His, if a subdiaphragmatic segment is created surgically - whether it be by a pulldown gastropexy a la Boerema, by a fundoplication, by inserting a silastic appliance a la Angelchik or by simply creating one out of stomach a la Collis - reflux will often be alleviated. This encourages another instance of the post hoc fallacy. Each of these procedures in some way interferes with vector resolution of the force of LMC: by creating a slack PEL (Boerema), by changing the angle of resolution (prosthesis), by extending the esophagus (Collis) or by destroying the PEL. The beneficial effects are not due to the intended rationale.
![]()
The physiologic lower esophageal sphincter
A major outcome of the manometric methods pioneered by Fike, Code, Ingelfinger
and their schools has been the nearly universal acceptance of the existence
of a physiologic sphincter of the lower esophagus.(21)
This was a giant step in the direction of understanding reflux even though manometrists
misplaced it and radiologists did not recognize it. Physiological research is
now concentrated on understanding the role of the sphincter in preventing reflux.
The understanding is presently hampered by a fundamental limitation of the instrumentation
employed: it is 2-dimensional due to its inability to "see" the LM.
A 1986 report by Dodds, et al.(22)(23)
illustrates the problem. This group measured the mean 12 hour lower esophageal
sphincter pressure in patients with clinical and esophagoscopic evidence of
esophagitis and in a control group without esophagitis. The mean pressure at
the LES in the control group was 29 9 mm of Hg. In the patient group it was
less than half as much - 13 9 mm. This suggests that a normal (high) average
LES sphincter pressure, thought to be a measure of the tone of the circular
sphincter muscle, prevents reflux. Yet, 4 of the patient group had mean 12 hour
LES pressures that fell in the normal range.
Also unexplained by the hypothesis that a normal LES tone prevents reflux was
the finding that transient complete LES relaxation occurred in both the control
and esophagitis patients. Even when the measured LESP was reduced to 4-5 mm
Hg, reflux did not always occur. In the controls, only 34% of those with complete
sphincter relaxations had reflux; the other 66% with the same transient
relaxations did not have reflux. In the patient group the results were almost
exactly the opposite: 2/3 of the relaxations were accompanied by reflux. In
short, there is a 33% overlap of controls and patients - 1/3 of those with normal
mean pressures reflux and 1/3 of those with low sphincter pressures do not.
On the other hand, administering a drug believed to increase LESP (metoclopramide
10 mg q.i.d.) produced no significant correlation between increased LESP and
decreased symptoms.(24)
Although there is evidence that 80 mm Hg pressure in the stomach will not force
the sphincter, Dodds et al. found that even a minimal LES pressure
of 4-5 mm Hg was enough to prevent reflux. The study showed that transient
complete sphincter relaxation is the cause of reflux - not low resting
LES pressure.
In an earlier study,(25) it was found that
reflux episodes tended to be "inappropriate." They might occur without any other
esophageal motor activity or with random, non-peristaltic activity. These results
were confirmed in dog experiments by Patricos, Martin, Dent et al.(26)
who also established that belching was initiated by a single transient complete
LES relaxation and that it did not occur as long as a measurable LESP existed.
Euler and Byrne(27) studied 49 infants and
children under 9 years with 24-hour pH probe testing. Although the symptomatic
and asymptomatic groups were sharply differentiated by the number of reflux
episodes and their persistence, there was no significant difference in LESP
between the two groups. (21.1 1.7 vs 21.7 1.7) Hillemeier et al.(28)
found normal or increased LESP in children under 2 years with severe
GER.
Despite the work of the Milwaukee group, clearly indicating that 1.) low LESP
per se is not the answer to the problem of reflux, and 2.) reflux is
due to transient complete sphincter release,(29)
great activity is focused on the physiology and pharmacology of the sphincter.
Earlam [1975] probably stated the consensus echoed in current texts(30)
when he said, "Since the pathology is most likely an intrinsic defect
of the gastro-esophageal sphincter and the lower esophagus, the ideal treatment
would be to tone up the sphincter and increase the efficiency of secondary peristalsis
. . . " [emphasis added]. Behar(31) after reviewing
the literature, concluded the causes of LES incompetence were unknown.
Sweeting(32) notes, "There is no adequate explanation for these seemingly random drops in sphincter pressure. None of the factors studied have been shown to be paramount in determining basal LES pressure."
![]()
The LES has been intensively studied both in vivo(33)
and in vitro. In his 1982 review, Diamant(34)
cites a large number of results. Cholecystokinin octapeptide (CCK-OP), for example
will decrease sphicter tone in the cat, but increases it in the opossum. It
has the reverse effect on both animals if the LES is chemically denervated with
tetrodotoxin (TTX). Progesterone lowers LES pressure during pregnancy or if
given as medication.(35)
Stimulation of the cut peripheral end of the greater splanchnic nerve increases
LES tone 300% in the cat but reduces it 50% in the opossum. Stimulating the
central end of the splanchnic nerve decreases LES pressure in both
animals. Significantly, CCK-OP decreases LES pressure in normal humans, but
increases LESP both in patients with diffuse muscle spasm and in those with
achalasia. CCK-OP has the same paradoxical effect on the cat after TTX(36),(37),(38)
However, it is hard to attach great weight to the finding because CCK-OP produces
a decrease in LES pressure in the chemically denervated opossum. CCK-OP
also causes ". . . forceful LMC" in the opossum.(39)
Clinically, "The poor correlation of LES hypotonia with reflux esophagitis
suggests that in many patients the occurrence of reflux is either determined
by nonspincteric factors or by features of sphincter activity other than basal
LES tone." (40)
It is difficult to interpret such findings, in part because of species variation, in part because some are done on intact animals and others on isolated preparations, but principally because LMC is not taken into account. An observed decrease in LESP, for example, could be due to LMC but undetectable with the instruments used. In studies on intact animals, if a single orifice manometer is used, the sphincter may be drawn up above the catheter orifice by LMC to create a false reading of decreased LES pressure. Without repeating the experiments, it is uncertain whether the LES pressure drop is due to the effect of the drug or stimulus on the sphincter muscle directly or indirectly via the LM.
![]()
Edwards(41) was unable to measure sphincter pressure after vagal stimulation because the "violent" contraction of the LM on stimulation of the vagus moved the sphincter off the manometer tip. There is no feasible way of obtaining quantitative measurements of LMC and LESP simultaneously in man. Harrington, et al.(42), using a more elaborate experimental setup in the opossum also found that vagal stimulation caused LM contraction and LES relaxation and that LESP was correlated with LM contraction and relaxation whether spontaneous or pharmacologically induced. The location of the sphincter in this animal is 5 cm below the diaphragm so this effect must have been purely neurologic and independent of the vector resolution of LM force by the PEL.
The demands placed upon the LES make it almost unique among sphincters. With
the exception of the cricopharyngeal sphincter, it is the only sphincter that
must function in the orad as well as caudad directions. It must pass fluids
and solids with a minimum of obstruction and yet be a firm barrier against the
incursion of the corrosive, not to say repugnant, contents of the stomach. It
must allow discharge of the air that is constantly being swallowed at a rate
of a few cc per minute, yet nip off the escaping gas before the swiftly approaching
gastric fluid level passes its portal. On occasion, nevertheless, it must yield
to massive discharge of gastric contents in vomiting while preserving its structural
integrity for immediate resumption of its normal function.
The integration of these functions with the circular and longitudinal muscular components of the esophagus in swallowing fluids, in swallowing against resistance and in belching has been described in the appropriate chapters. Here we are concerned with a malfunction in which the LES is open when it should be closed. It would be very strange if this pathological opening of the LES were not due to the same force that opened it physiologically in swallowing, belching and vomiting. Like people, whose faults are rooted in the same qualities as their virtues, malfunction is of a piece with physiology.
![]()
LMC and reflux
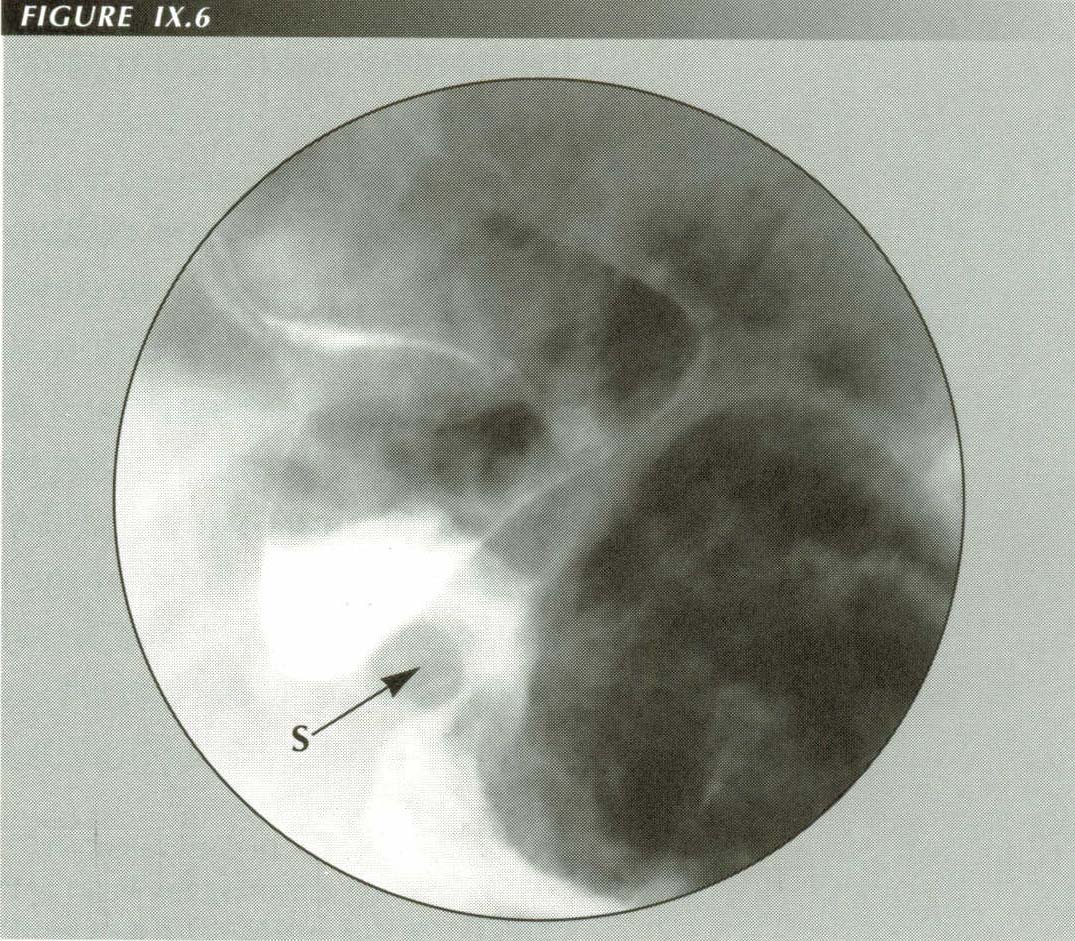
Briefly stated, my thesis is that increased LM tone is responsible for GER.
LMC -->
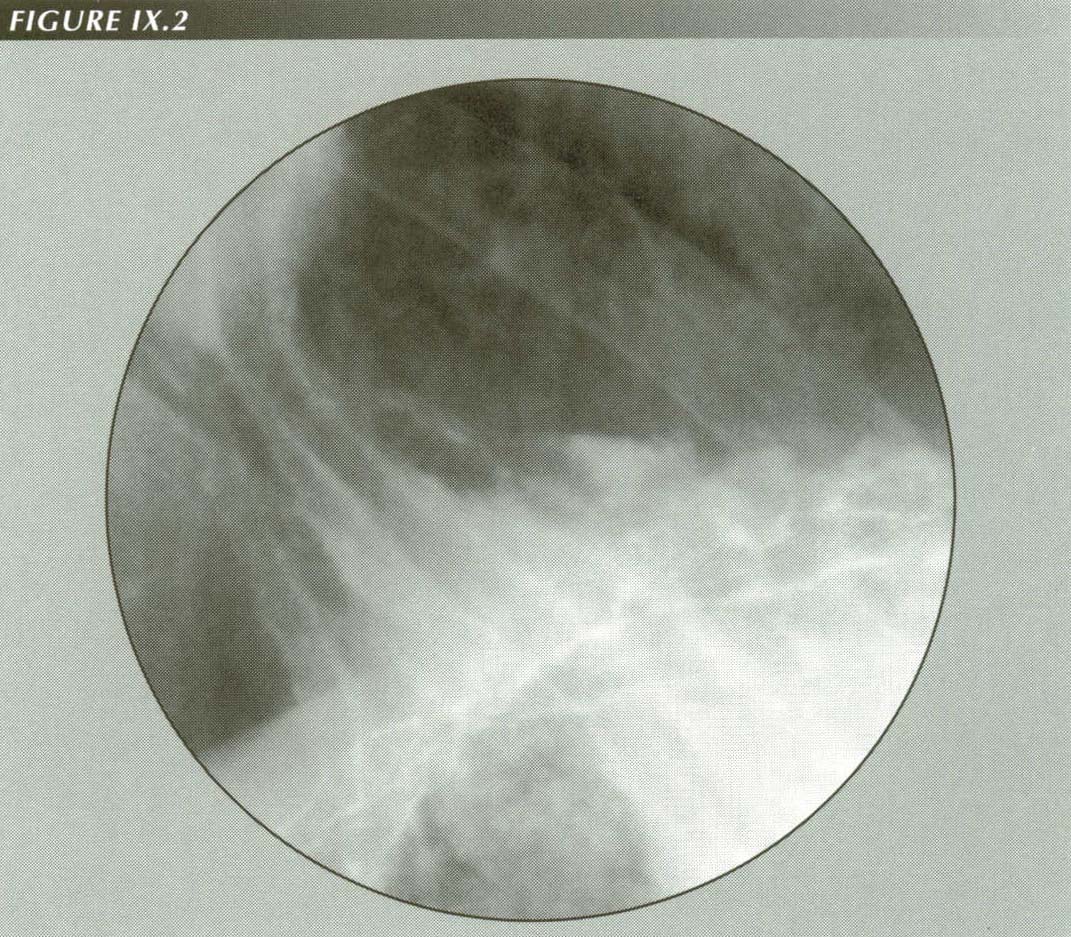
LMC produces reflux: LMC is evident from the marked tenting of the fundus into an unusually wide hiatus. The lateral stretching of the GE junction explains the fact that, although produced by longitudinal traction, Mallor Weiss tears are also longtudinal. Barium in the distal esophagus is reflux. The hiatus itself is widened by the lateral resolution of LM force. If a transducer is measuring hiatal squeeze, it will register decreased pressure when the LM contracts!
Before integrating the LMC mechanism with the Cannon-Dougherty reflex (CDR),
it is appropriate to review the evidence that LMC can or does open the sphincter.
The main points can be listed:
GER is a component of the tetrology of HH, LER, tertiary contractions and
reflux. The mutual associations favor a common cause. I have shown or will show
that LMC causes HH, LER and TC.
In scleroderma, a disease in which the esophagus is shortened, there is gross
GER and HH.
LMC must occur before sphincter release in belching.
Forceful LMC occurs with sphincter release in vomiting.
Observation of patients swallowing against resistance shows that LMC is an
integral part of the peristaltic wave. LM contraction during the phase that
the sphincter is open and its relaxation synchronously with sphincter closing
are meaningless unless the LM has a sphincter-opening function.
The experiments of Torrance(46) demonstrated
that the LMC induced by vagal stimulation produced reflux whether or not the
sphincter was denervated. H. Daintree Johnson(47)
found similar responses in the rabbit. Like Torrance, he found that simple traction
on the esophagus through a neck incision caused a gaping cardia.
Vector resolution of the force of LMC opens the sphincter by pulling the opposing
surfaces apart. This is a purely mechanical result independent of the pharmacology
or neurophysiology of the sphincter, so that we can say, If the LM contracts
and the PEL is intact then sphincter-opening vectors will inevitably
be generated.
When PEL rupture converts a sliding HH to a "paraesophageal" HH the force
vector cannot be resolved and reflux is relieved. This is why the giant HHs
in the elderly are generally asymptomatic.
All operations that alleviate reflux do so by destroying the PEL or changing
its direction thus impairing the ability of the PEL to resolve LMC into a sphincter-opening
force.
Non-effacement of the sphincter is a frequent consequence of PEL rupture.
Fluoroscopic observations of belching, nausea and vomiting demonstrate that
LMC is associated with these sphincter-opening events.
Disabling the LM by drugs or surgical trauma can relieve symptoms caused by
reflux.
In myotonia dystrophica, a disease in which the LM cannot relax normally after contraction, the sphincter may be always open with a resulting air esophogram.(48),(49),(50)
![]()
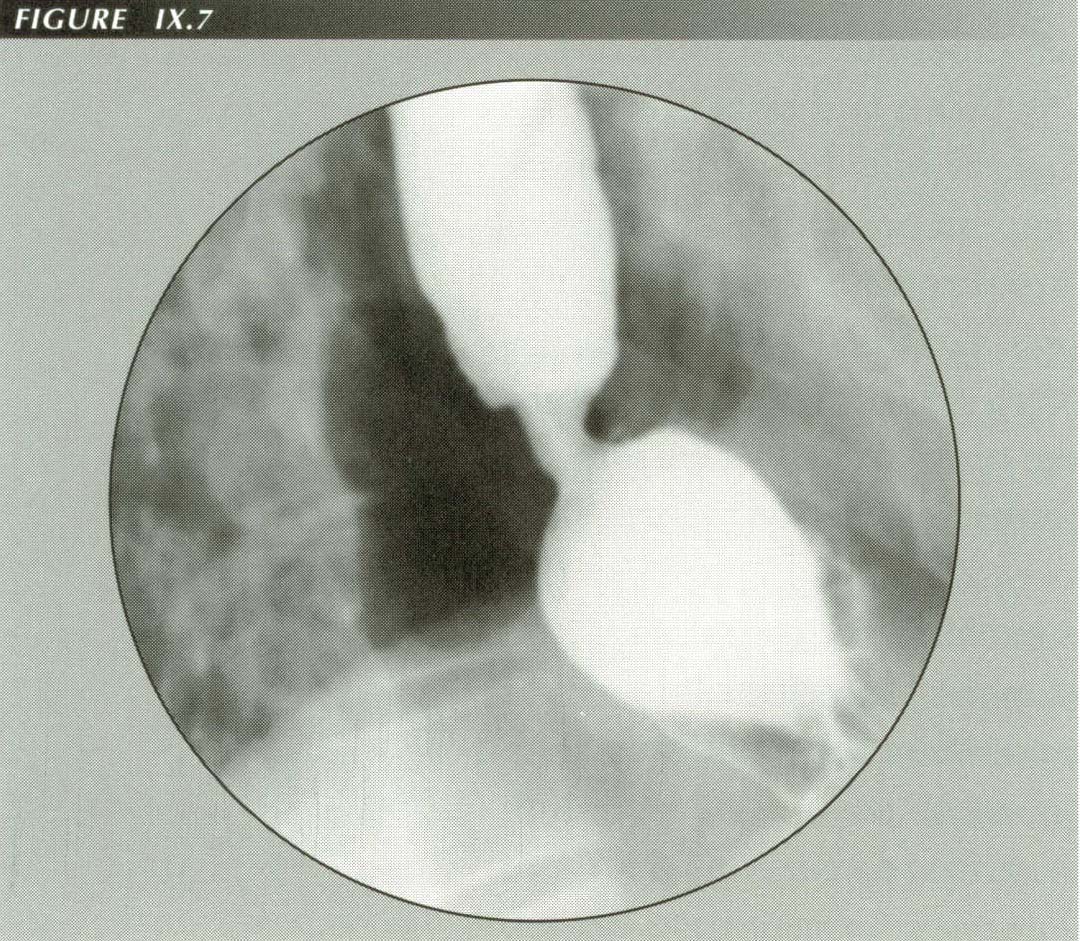
Shortening the esophagus causes reflux.
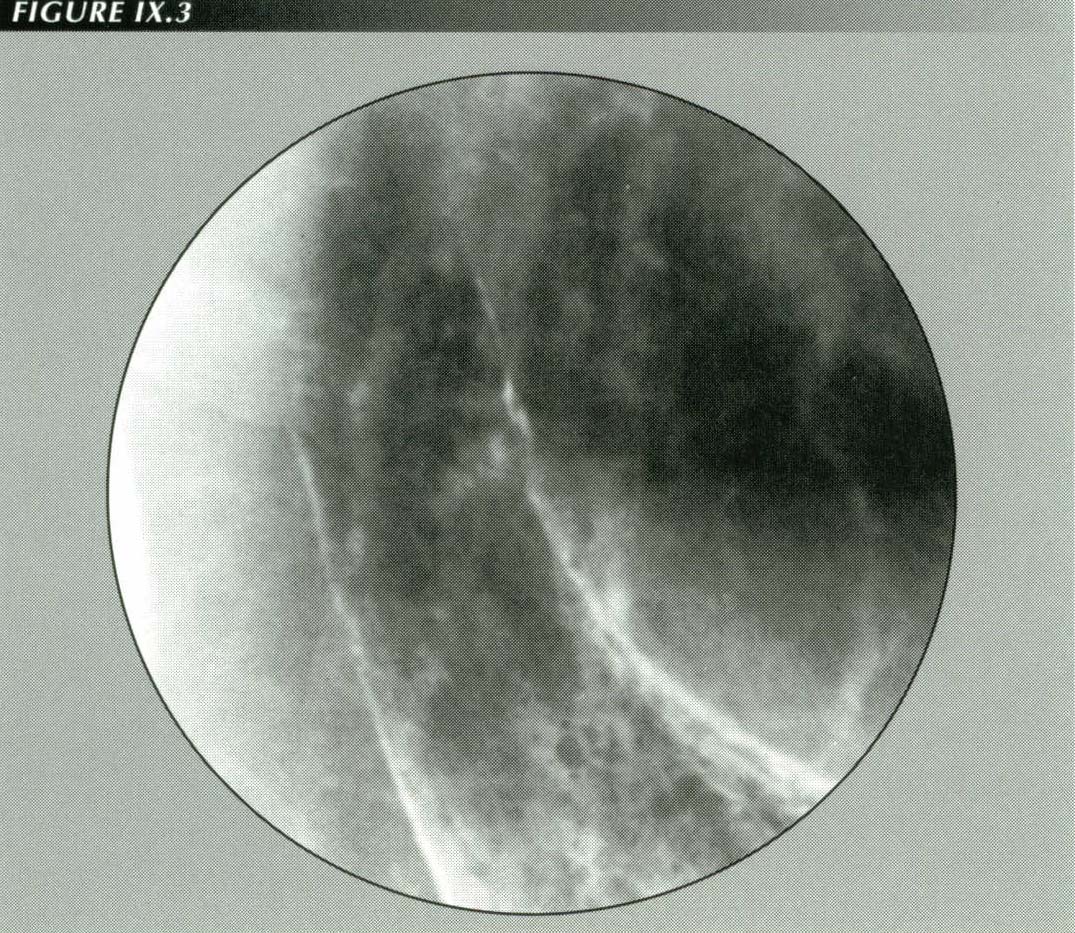
LMC opens the sphincter: In some extreme cases of excessive LMT the sphincter may remain open indefinitely as in this patient. The trumpet shape is the geometrical resultant of resolution of the force of LMC into sphincter- opening and PEL- stretching components. Receptors in the fundus, when stimulated by acid/pepsin, inhibit LMC. The appearance seen here may be reproduced by washing the posterior wall of the stomach with water (the de Carvalho maneuver) thus �turning off� the inhibitory reflex.
Vanhoutte et al.(51) studied whether
the reflux was due to interference with peristalsis. They found that resection
of 2 cm of the esophagus in newborn dogs did not result in a loss of the peristaltic
wave below the resection site. Their speculation that the postoperative complications
were due to a ". . . . coexistent congenital abnormality of the vagus nerve."is
tantamont to an admission of ignorance. Jannsens has demonstrated that the peristaltic
wave also survives vagotomy.(52)
The complications of TEF repair are such that the operation is a human experiment
in producing the syndrome of LM tension. The traction on the lower esophageal
segment necessary to approximate the transected esophagus after removal of the
atresia can and does cause the three complications of excessive LM tension -
strangulation, hiatus hernia and reflux. Although experimental esophageal transection
does not produce motility disorders in the dog,(56)
opossum or rhesus monkey,(57) a motility disturbance
that resembles diffuse spasm (tertiary contractions) and dysphagia for solid
food frequently complicate TEF repair in later life(58)
because of the esophageal shortening.



Indeed, any anomaly that applies traction to the PEL may result in an open
sphincter. Vascular rings that elevate the esophagus often cause an air filled
esophagus with an open sphincter.
Lengthening the esophagus alleviates reflux.
The most severe cases of reflux are those with esophageal strictures. Resection of a portion of the esophagus, e.g., for stricture, shortens it and leads to recurrence. If, however, the esophagus is lengthened by the Collis(60) procedure, the success rate is reported to be 75% despite what is essentially surgical creation of a Barrett's esophagus.(61) Even these failures can be treated by interposition of a segment of left colon or jejunum.(62) Clearly, just as shortening of the esophagus promotes reflux, lengthening it counteracts reflux by relieving its tension.
![]()
Coordination of sphincter, CD reflex and LMC
Given a normal range of LM tone, for the sphincter to open, the Cannon-Dougherty
reflex (CDR) must be OFF. This is a necessary, but not sufficient condition.
The LM must be ON. Three of the components of GER - LM, sphincter, and the CDR
- can be arranged in a Truth Table (Table 1).
A simple "circuit" controls the sphincter when all is well: it is closed unless
the CDR is turned OFF and the LM is turned ON. Note that this control
scheme does not give the sphincter itself any place as a prime mover. It is
completely under the joint control of the LM and the CDR.
This schema is not in conflict with the extensive studies of the pharmacologic
control of sphincter tone; reflex control must to be mediated via neurotransmitters
in any case. The effect of LMC, however, appears to be primarily mechanical.
The sphincter snaps shut as soon as LMC stops.
Sphincter control is not entirely an all or none affair regulated in digital
fashion, at least as far as the LM is concerned. Given an intact PEL, the LM
can always open the sphincter if only it contracts forcefully enough.
TABLE 1
Truth table for the lower esophageal sphincter
| CDR | LMC | SPHINCTER | Effect |
| OFF | OFF | CLOSED | Baseline tone closes sphinct. |
| OFF | ON | OPEN | LMC opens sphincter |
| ON | OFF | CLOSED | CDR prevents opening |
| ON | ON | CLOSED | CDR prevents opening |
![]()
Diagnosis of reflux
Many studies of reflux are needlessly complex, uncomfortable and expensive.
Leasing the equipment for pH monitoring can run several hundred dollars a day.
The radiologic diagnosis of reflux can be highly specific and uncomplicated.
At the moment the de Carvalho maneuver elicits reflux one simply asks the patient
four questions:
1. Do you feel anything unusual?
2. Have you had that sensation before?
3. Is this like the symptom that has been bothering you except in degree?
4. Is it in the same place as that symptom.
Four "yes" responses leave yield more certainty that reflux is the cause of
the patient's symptom than any strip chart. As usual, there are caveats. Negative
responies do not exclude reflux. If too much water is used to elicit reflux,
gastric HCl may be too dilute to elicit the symptom. A few patients with life-long
reflux are so accustomed to it they believe it is normal.
The association of hiatus hernia and reflux
"Most physicians have for many years associated . . . gastroesophageal reflux
with an anatomical hiatus hernia."(63) In a
typical report, Edmunds(64) found radiologic
evidence of reflux in 93% of sliding HH and 42% of "rolling" HH's. Wright and
Hurwitz(65) compiled a chi-square table of 293
patients calculating that the probability that the association between HH and
esophagitis was due to chance was less then 1:10,000.
| HH + | HH - | |
| Esophagitis + | 32 | 6 |
| Esophagitis - | 32 | 223 |
The notion that a 2 with a low P proves causality dies hard. Because
of the association, it was it was natural to assume that one caused the other
so this view prevailed. As recently as 1994 Paterson and Kolyn,(66)
based on their finding that acid perfusion of the opossum esophagus caused it
to shorten, conjectured that esophagitis caused HHs. As a result, HH repair
enjoyed a long vogue as the accepted treatment for GER.
As the repairs were often less than satisfactory, surgeons directed their efforts
toward designing operations that would deal with reflux per se and
not simply correct a HH as before.(67) Nevertheless,
the strong association remains - with a difference. It can no longer be attributed
to cause and effect, but, if it is not cause and effect, why the association?
Dodds, et al., however, suggested, "Perhaps hiatal hernia and GE reflux
are related to a common cause rather than being related causally to each other."(68)
The hypothesis we are proving nicely solves the dilemma as it shows that HH
and reflux occur together because, as Dodds suspected, they do have
a common cause, LMC. Looking at it from the opposite way, this association further
proves the validity of the sphincter opening mechanism. If there is long continued
excessive LM tension sufficient to cause stretching of the PEL (i.e., gastric
transtraction) one would expect that there would also be excessive sphincter
opening activity (i.e., reflux).
One cannot completely rationalize the considerable complexity of sphincter
control with a one-factor mechanism. It seems that there are at least six and
probably more factors involved:
The sphincter-opening force generated by LMC
The ON/OFF status of the Cannon Daughterty reflex.
Whether the contractile mode of the LM is peristaltic, tonic, clonic or anaspartic.
The integrity of the PEL.
The basal tone of the sphincter
The contents of the stomach
It will take a more powerful LMC to open the sphincter if the CDR is ON or if there is a high intrinsic sphincter tone. We can see this in the events that preceded a belch. LMC will tent the PEL, then subside without an actual release of gas then again contract, perhaps with a more pronounced tenting as the cone of gas elongates into the sphincter region. In emesis mode, of course, such is the power of the LM, the sphincter is forced even if the CD receptor is activated.
![]()
The role of gastric contents in reflux.
We can belch without regurgitating acid because as soon as the gastric fluid
level reaches the CDR receptor, the LM is inhibited and the sphincter closes.
Watching this process with the fluoroscope, one has to wonder how a reflex mediated
by a chemoreceptor can be so quick.
Production of gastric mucus can explain both the delayed onset and the intermittent
nature of heartburn related to ingestion of certain foods. As the CDR receptor
must be stimulated chemically, mucus coating the stomach will prevent gastric
acid-pepsin from contacting the sensor and activating an inhibitory reflex.
Non- effacement of the sphincter: The PEL is ruptured in this patient with 50% of the stomach in the chest destroying the normal mechanism for sphincter effacement. The sphincter may be pylorus-like as in this case, neither opening or closing. This may cause mild dysphatgia. The 1 cm sphincter length is far shorter than the 4.5 cm or more derived from manometry.
If it could be shown that carminatives cause excessive mucus production this
would tend to show that they cause heartburn by coating the CD receptor with
mucus and so suppress the CD reflex sphincter closure. The delayed (45-60 minutes)
effect of these substances in promoting reflux(69)
would fit this mechanism. It also is a rationale that accounts for the paradox
of an irritant causing sphincter relaxation.
Bickel and Kauffman(70) developed methods of
measuring the thickness of the gastric mucus layer. They found that distention
of the stomach stimulated release of mucus. "The gel mucus layer overlying the
gastric mucus is constantly being produced by the surface epithelium and is
constantly being eroded within the lumen by the action of acid, pepsin, and
stirring of the luminal fluid." The application of certain substances such as
prostaglandin E2 could increase mucus thickness.
In theory, there are other ways of turning off the CDR. Local surface anesthesia
produced that effect in ruminants(71) as did
section of the dorsal trunk of the vagus. Ingestion of a surface anesthetic
may explain the effect of procaine noted by Balfour.(72)
The deCarvalho maneuver or water siphonage test turns off the guard reflex by
washing it free of acid-pepsin. Released of the reflex inhibition, basal LM
tone overrides basal LES tone.
It could also be true that a more complex set of receptors feeds a central program that calculates gastric shape. A sudden loss of distention on release of gas from the stomach would then signal the LM to relax.
![]()
The cervical spine and reflux
It will be recalled that an elevation of the mouth of the esophagus initiates
a swallow thus applying tension to the entire esophagus and through it to the
PEL thus facilitating opening of the sphincter.The upward impulse of the larynx
that initiates a swallow may also activate a stretch reflex causing further
contraction of the LM. In drinking liquids this and gravity are all that are
required. Usually no peristaltic wave results except as a final cleanup.
If increasing LM tension facilitates sphincter opening, it is worth considering
whether decreasing LM tension would improve sphincter competence thus decreasing
the amount or frequency of reflux. In principal, it would seem that ceteris
paribus, shortening the distance between the ends of the esophagus should
relieve the tension on its attachments. This can be done very simply by anteflexing
the cervical spine.
Although unintended, cervical anteflexion is invariably a part of the standard
treatment for reflux. Without exception, authorities advise sleeping with the
head elevated. Effectively, this is a prescription for cervical anteflexion.
Typically, a patient is told to sleep with his/her head elevated.(73),(74),(75),(76),(77),(78),(79)
The physician assumes that the patient will elevate the head of the bed with
bed blocks as is done in hospitals. The patient however, thinks he/she
has been told to sleep on two pillows, does so and gets relief! They would get
as much relief by sleeping on a 28" x 10" foam wedge.(80)
There is no rationale for bed blocks
The only conceivable rationale for suppressing reflux by elevating the head
of the bed is to affect hydrostatic pressure gradients. We accept that explanation
because we are aware we are doing something right(81)
and nothing else comes to mind.
A elementary calculation with similar triangles shows that elevating the head
of the bed does not change the hydrostatic pressure differential more than a
few cm(82) of water. It takes 80 mm Hg or more
of hydrostatic pressure to force the sphincter, so .28 mm Hg is not going to
tip the balance in favor of sphincter competence. Moreover, even 6 inches of
elevation makes people slide out of bed and is likely to be objectionable to
a patient's spouse. The bed-raising may tend to get the CDR receptor out of
the pool of gastric secretions, but this should promote reflux. Moreover,
the esophagus is bowed posteriorly by the heart so that this slight adjustment
makes no difference.
Curiously, people have reflux even when the pressure differential is maximized
in the upright position. In a study of 100 patients with and without HH, Johnson(83)
found that the number of episodes of reflux per hour was three times as
great in the upright position as in recumbency! So elevating the head should
promote reflux! How can one explain such a paradoxical result by hydrostatic
pressure? Even if it were just a matter of acid pouring out of the fundus through
an open sphincter, it would be paradoxical. The universal medical recommendation
to sleep with the head elevated is a remarkable triumph of empiricism over logic.
On the other hand, anteflexion of the cervical spine occurs in recumbency on
pillows. This explains the favorable effect of this advice and Johnson's results
become predictable. The prescription works because the doctor's instructions
are either misunderstood or tried and, after being found intolerable, no nurses
being around to enforce them, modified. Cervical anteflexion can introduce nearly
the same amount of esophageal slack as a Collis procedure and is effective for
the same reason.
An unsolicited testimonial for this rationale is provided by Garretts,(84) who, in reported apthous-like denudations on the buccal surface of the lower lip in three patients with reflux, mentioned that the second of these dated his symptoms to a fall in which he hurt his neck. Thereafter, he "...could not use his usual number of pillows..." but had to sleep lying flat in bed. He was advised to raise the head of the bed!
![]()
A useful maneuver
Those readers occasionally afflicted with reflux may test these conclusions
on their persons on such occasions by firmly forcing their chins down toward
their chests. A measure of relief may be experienced almost at once. While the
maneuver is not a miracle cure, it can make the difference between going back
to sleep and a trip to the medicine cabinet.
This maneuver is about equally effective - and for the same reasons - in suppressing a wave of nausea or an incipient belch. A patient may be able to ward off an attack of angina-like chest pain with the maneuver.(85) As a rule, the body knows how to adjust its position so as to minimize discomfort. It is surprising, therefore, that this is not a posture that everyone discovers for himself as, for example, most people discover that leaning forward and hyperextending the cervical spine will facilitate a belch.
![]()
Cervical dorsiflexion can cause reflux.
Just as anteflexion seems to slack off the LM and alleviate its sphincter-opening
effects, there is a remarkable association between dorsiflexion of
the cervical spine, contraction of the LM of the esophagus and reflux. As might
be expected, it has precisely the opposite effect. It tends to open the sphincter.
The following 4 cases (for 2 of which only my notes survive) illustrate the
extent to which dorsiflexion causes a striking degree of LMC.
An opportunity to observe LMC in its severest form was furnished by an extraordinary
patient, male, age 36 who was seen for dysphagia, choking, laryngospasm, heartburn,
etc.
With each swallow, the LM contracted en masse producing a trumpet
configuration of its lower segment, herniating the stomach and opening the sphincter.
The latter remained wide open for more than 30 seconds at a time. As the hernia
started to reduce, the sphincter would begin closing, only to reopen as an increase
in the force of LMC again elevated the stomach above the diaphragm. A further
finding of interest was the accidental discovery that to provoke this "tetanic"
LMC, it was only necessary to hyperextend the cervical spine. This maneuver,
of course, put the esophagus on stretch and elicited the LMC response just as
an abrupt flexion of the ankle can produce clonus.
On review of the cine film of the case, one is impressed with the strength
and elasticity of the PEL that can withstand a force of this magnitude without
rupture and without loss of elasticity.
The chief significance of this unusual case, seen in the early 1960s was that
it illustrated an extreme degree of LMC and thus made it easier to recognize
lesser degrees of the same condition in others.
CD/40585 This 45 year old male exhibited many signs of a hyperactive, hypertonic
LM. The presence of a trumpet shaped HH, gross, spontaneous GE reflux and marked
reflux in response to the de Carvalho maneuver were all considered manifestations
of this primary abnormality. The esophageal sphincter remained open for long
periods even in the upright position so as to suggest scleroderma initially.
Dorsal flexion of the neck produced reflex contraction of the esophagus bringing
on the above effects.
An even more striking example, for which I have been unable to find a comparable
report in the literature, was seen a few years later.
The patient was a man in his 20s who was brought to the department in what
appeared to be a bizarre type of convulsion. Extreme cervical hyperextention
occurred spasmodically as the patient thrashed about on the x-ray table so violently
it required several aids to keep him from falling off. He was able to cooperate
in swallowing barium, but his motions were so erratic the lower esophagus could
not be retained in the 4"x 5" field of the cine camera.
The barium-coated esophagus was alternately air filled and collapsed. The filling
occurred when he hyperextended his neck. At this time the esophagus contracted
longitudinally opening the sphincter and allowing air to escape into the esophagus.
This would be followed immediately by an en mass contraction of the
circular muscle or Valsalva effort that forced some air back into the stomach.
These activities were accompanied by loud eructations of gas via the superior
constrictor as well.
Such dramatic instances are not necessary to demonstrate the effect. It can
be seen in almost any patient with reflux and/or HH.
A 59 year old schizophrenic with severe esophagitis and HH was studied. When
an assistant dorsiflexed the cervical spine, the HH could be seen moving up
and down in the hiatus. Reflux occurred at maximal dorsiflexion.
In all these cases, one had the impression that there was a "knee jerk" reaction such that stretching the LM by dorsiflexion induced contraction just as a percussion hammer, by stretching the quadriceps tendon, causes reflex contraction of the extensors of the knee.
![]()
Sandifer's syndrome
Also noteworthy in this connection is the equally bizarre Sandifer's syndrome
seen in children. It is marked by head rolling, hyper-extension of the cervical
spine, hiatus hernia and reflux.(86),(87),(88)
The children began the movements during eating and seemed to get some relief
from them. They were not present during sleep. The preferred posture was supine
in bed with the head hyperextended over the edge of the bed like the comic strip
character Lou Ann. They learned to watch television upside down in this position.
All had HH with reflux and vomited at mealtimes. Radiological examination of
5 such patients including Sandifer's by Sutcliffe established that the fundus
of the stomach was elevated and the HHs sharply increased in size with the dorsiflexion
movements. "The stomach would bob up and down in time with the neck movements."
"The neck contortion would immediately be followed by substantial elevation
of the GE junction and temporary entry of a further portion of gastric fundus
into the thoracic cavity."
Although the movements were so bizarre they suggested basal ganglia disease,
they cleared completely after hiatus hernia repair!(89)
A later series of 13 cases mimicking other neurological syndromes was reported
by Bray, et al..(90) Most were infants
with torticollis, opisthotonic posturing and seizures whose symptoms cleared
with postural treatment of their reflux and HH'S. As all of the children either
had dysphagia or vomited at mealtimes, it seemed that there was some obstruction
of the esophagus that putting the esophagus on stretch relieved. This would
have the same sphincter-opening effect as would LMC.
On followup of 31 patients with mental motor retardation who had been subjected
to Nissen fundoplication for severe GE reflux, Williams and associates(91)
reported that the only factor of prognostic significance in predicting a poor
result was " . . . chronic opisthotonic posturing . . . " that occurred in 80%
of failures. Like Sandifer's syndrome, such a posture forces severe cervical
hyperextension causing esophageal traction.
Such cases establish the connection between esophageal tension and both HH and reflux and show how movements of the neck affect the lower esophagus. They provide a convincing demonstration that cervical dorsiflexion can produce HH by esophageal traction and that the same LM tension is associated with reflux.
![]()
"Whiplash dysphagia"
Orthopedic surgeons have long been mystified that their whiplash patients have
dysphagia. I examined three such patients who complained of heartburn and lump
in the throat. Although under 35, they had HH's with ruptured PEL's. The hyperextension
of whiplash injuries exerts enough sudden stress on both the proximal and distal
attachments to rupture the latter and cause local injury to the cricopharyngeus.
Diaphragmatic paralysis for reflux
The "knee-jerk" analogy may also explain the success reported treating reflux
by phrenic nerve crush in patients considered poor risks for major surgery.
Relying on conventional doctrine, surgically paralyzing the diaphragm seems
so lacking in rationale that Earlam cites it with unconcealed skepticism: "
. . . if the results are to be believed - paralysis of the diaphragm on the
left side does, for some unknown reason, relieve symptoms."
But paralyzing the left hemidiaphragm also gives the esophagus a few centimeters of slack - perhaps as much or more than cervical anteflexion - and this in turn takes the strain off the PEL preventing a stretch reflex in the same way that extending the knee diminishes a knee jerk. Seen in this light,(92) phrenic nerve section is just as rational as sleeping on 2 pillows or a pulldown procedure or lengthening the esophagus.
![]()
Esophageal slack reduces reflux
Non effacement of sphincter with ruptured PEL. The sphincter- opening vectors generated by LMC require resolution by the obliquely inserted PEL. Such cases are often labeled �terminal esophagitis.�
The Collis procedure, an anti-reflux operation in which a tube is fashioned from the stomach to provide what is in effect an esophageal extension, is said to be effective because it " . . . eliminates tension on both the repair and the intrathoracic esophagus."(94) Again, elongating the esophagus has the effect of reducing the tension it can apply to the PEL.
![]()
PEL rupture alleviates reflux
Elongating the esophagus, flexion of the cervical spine and raising the stomach
all achieve their effect by reducing the LM tension on the PEL. There is, however,
still another way of reducing the sphincter-opening potential of the LM. Because
vector resolution of the force of LMC by the PEL opens the sphincter, transecting
the ligament should destroy this resolution thus alleviating reflux. Then LMC,
no matter how forceful, would be ineffectual at producing reflux.
The patient in the following case had a symptomatic remission after a sliding
HH converted to a non-slider:
25117 AC, M age 69. On 10/21/63 the patient had a sliding HH, gross reflux
and a lower esophageal ring. Then he had genuine dysphagia (i.e., not lump in
the throat), pain in the right side of the chest and interscapular region as
well as symptoms of regurgitation. On the present occasion, all these symptoms
have cleared and the patient states he has been asymptomatic for the last 3
months. 10/18/65
Fluoroscopic note: Barium passed freely through the esophagus. The GE junction
was 7.5 cm above the diaphragm. Although there was a pinchcock-like appearance
at the diaphragm on straining, this was not tight enough to prevent barium from
leaving the herniated portion of the stomach idicating rupture of the PEL. The
hernia had increased in size by a factor of 100% and the LER, that formerly
had fairly sharp, ledge-like margins, on this examination had blunt, lip-like
margins.
Although no operation is limited to simple severance the PEL(95),
nature has provided an experiment that verifies the above prediction. Many cases
of GER are eventually self-limited. It is common experience that the huge HH's
seen on admission chest films of the elderly are often asymptomatic. Barrett(96)
does not even list pyrosis among the complications of the "paraesophageal HH."
Johnstone's comment on the origin of the angle His theory of GE competence will
be recalled. The large "rolling", "paraesophageal" hernias were so asymptomatic
that surgeons began to mimic their features surgically.
With age and a loss of elasticity, the PEL can rupture, converting what was
a slider to a non-slider, molar tooth, type HH. After this the force of LMC
can no longer be resolved in such a way so as to open the sphincter. LMC merely
shortens the esophagus, pulling anything attached to it through the hiatus.
This is the reason that so many patients with very large HH's are asymptomatic:
rupture of the PEL has pulled the LM's sting.
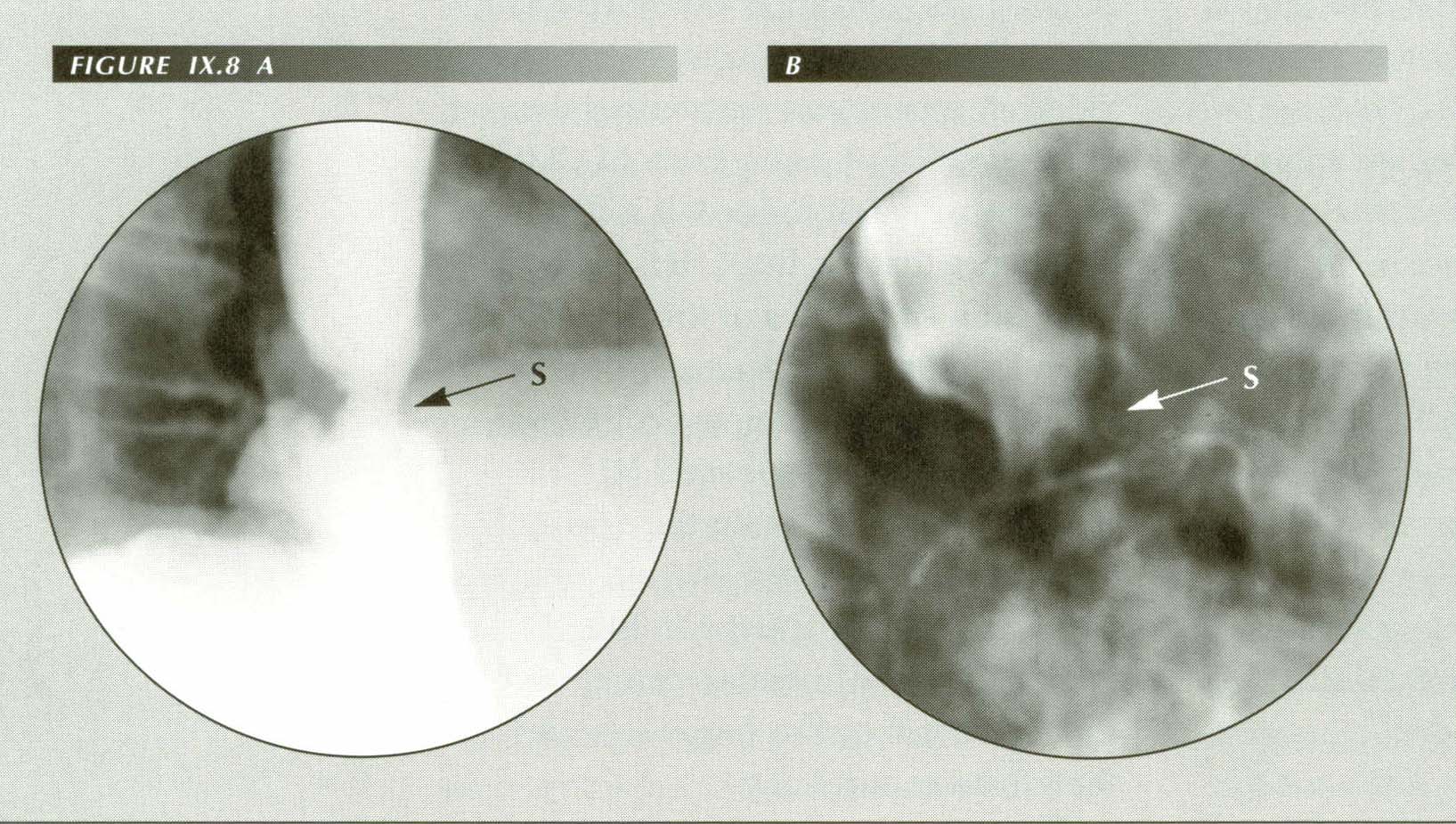
Non effacement of sphincter: Rupture of PEL demonstrated (A) by the dC maneuver, and (B) by inducing belching. The force of LMC is rerslved into sphincter-opening vectors by the PEL. When it ruptures this mechanism fails giving the appearance that Schatzki attributed to �terminal esophagitis�. It is actually a non-effaced sphincter. A mild dysphagia may result.
Patients with ruptured PELs do not escape entirely unscathed, however. As would
be predicted, without the assistance of the PEL they may have a problem effacing
the sphincter. Radiologically, the distal few centimeters of the esophagus present
as a short tapered segment or ring like narrowing that does not dilate with
rapid swallowing of large barium boluses. The result may be a mild to moderate
dysphagia. Many cases now labeled "terminal esophagitis" are probably examples
of non-effacement of the sphincter.
Finally, as has been noted in the hiccup chapter, a sudden downward motion of the diaphragm will release the sphincter by tensing the PEL. This explains the association of reflux with hiccups.(98)
![]()
SUMMARY
Gastro-esophageal reflux is the commonest of all gastrointestinal disorders.
Because the physiologic sphincter is the sole defense against reflux, its proximate
cause is sphincter incompetence. Its fundamental cause, however, is the excessive
tension on the PE ligaments that is commonly produced by increased tone or activity
of the LM of the esophagus. The PEL resolves the force of LMC into two components.
One component stretches or even tears the PEL, leading to hiatus hernia. The
other opens the sphincter causing GER.
Whatever tenses the esophagus promotes reflux. Shortening incident to repair
of TEF's results in postoperative aspiration pneumonitis. Contraction of the
LM opens the sphincter in swallowing, belching, gagging and emesis. Reflux is
associated with HH, tertiary contractions and LER's, not because of these conditions
per se, or the way they distort the anatomy of the lower esophagus,
but because all four of them are attributable to the same cause - esophageal
shortening by LMC.
In the rare disease, myotonia dystrophica, in which the LM cannot
relax, the sphincter, although not itself defective, remains constantly open.
It is tension on the PEL, not LMC per se that causes reflux. Thus,
hyperextension of the cervical spine or surgical shortening of the esophagus
- both of which apply traction to the PEL - also cause reflux.
Whatever relieves esophageal tension alleviates reflux. Disabling the LM by
surgical trauma, drugs or anesthesia will counteract reflux because these means
decrease LM tension on the PEL. Surgical elongation of the esophagus and anteflexing
the cervical spine are effective by the same mechanism.
With advancing age or forceful vomiting, rupture of the PEL may cure reflex
spontaneously, but non-effacement of the sphincter may then produce dysphagia
and an appearance easily mistaken for terminal esophagitis.
Sphincter opening depends on a balance of forces: the LM tension, the integrity
of the PEL, basal LES tone and whether the Cannon-Dougherty reflex is activated
or not. Even the 2.2 cm of slack created by anterior flexion of the cervical
spine may ameliorate symptoms of reflux, gas and nausea.
The cause of reflux is not intrinsic to the LES. Nor is it likely that an extrinsic
substance inhibits it. The details of its pharmacology are most relevant in
that they provide a clue to the action of the LM. A major implication of this
analysis is that investigation of substances that stimulate the LM is likely
to be more fruitful in eliciting a chemical cause of reflux. Compounds that
inhibit the LM are most likely to be of therapeutic value.
LMC, invisible to Flatlanders, is the unseen event that causes "inappropriate"
or "transient complete sphincter relaxation" in belching and reflux.
This is why low LESP alone does not cause reflux. This is why stimulating the
pharynx(99),(100)
(provoking LMC via a gag reflex) causes reflux. This is why the unguarded moment(101)
or failed peristalsis (LMC without a p-wave) causes reflux; why hiccups (the
vector equivalent of LMC) and tertiary contractions (LMC + CMC) cause reflux.
Normal swallowing (p-wave + LMC) would also cause reflux, were it not that
the advancing p-wave is a temporary sphincter that prevents backflow while it
is in motion and then merges the LES.
Pull-down type operations have a better rationale than procedures that attempt to reconstruct the angle of His or create a subdiaphragmatic esophageal segment - features not normally encountered in the living subject. These procedures apply countertraction to the force of LMC and by relieving tension on the PEL prevent a sphincter-opening vector resolution. Increasing esophageal length, severing or elongating the PEL or changing the direction of vector resolution can all be expected to have a beneficial effect.
![]()
References
Last Updated July 30, 2007 by David PJ Stiennon
1. 1. Alsop, Ronald, "New Alka-Seltzer ads revert to the humor of heartburn." The Wall Street Journal, page 33, November 11, 1985
2. 2. Douglas, R. Gordon, Jr., The common cold -- relief at last? N.Engl. J.Med. 314:114-5, 1986.
3. 3. DeMeester, T.R., Pathophysiology of gastro-esophageal reflux. In: Disorders of the esophagus: advances and controversies. Eds. Watson, A. and Celestin, L.R., Pitman Publishing, Ltd., London, 1984.
4. 4. Leonardi, Howard K. and Ellis, F. Henry, Jr, Complications of Nissen Fundoplication. Surg. Clin. N. Amer. 63:1155-65, 1983.
5. 5.Dodds, Wylie J. and Hogan, Walter J., Measurement of LES pressure. Gastroenterology 79: 588-91, 1980.
6. 6. Gunn, J.W.C., The carminative action of essential oils. J. Pharmacol. Exp. Ther. 16: 39-43, 1920. Cited by Earlam, Richard, Clinical tests of oesophageal function, Grune & Stratton, New York, 1975.
7. 7. Johnstone, A.S., Reflections on hiatus hernia and related problems. Radiology 62:750-3, 1954.
8. 8. Behar, Jose, Gastroesophageal reflux disease and its complications with a critical analysis of treatment. In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
9. The angle of His is believed to elevate a flap of gastric mucosa called the "Valve of Guberoff" but this also is a postmortem artifact.
10. 9. Johnstone, op cit.
11. 10. Friedland, Gerald W., Historical review of the changing concepts of lower esophageal anatomy 430 B.C. - 1977. Radiology 131: 373-388, 1978.
12. 11. Ziano, C., Poppel, M.H., Jacobson, H.C., Lepow, H and Osturk, C.H., Lower esophageal vestibular complex: anatomic- Roentgen study. Am. J. Roentgenol., Rad. Therapy & Nuclear Med. 84:1045-55, 1960.
13. 12. Hayward, John, The phreno-oesophageal ligament in hiatus hernia repair. Thorax 16:41-5, 1961.
14. 13. Groszek, Irena and Matysiak, Wlodzimierz, J., Morphologie der phreno-oesophagealen Membran. Gegenbaurs morph. Jahrb. 131: 1-18, 1985.
15. 14. Bombeck, C. Thomas, Dillard, David H. and Nyhus, LLoyd M., Muscular anatomy of the gastroesophageal junction and the role of phrenoesophageal ligament: autopsy study of sphincter mechanism. Ann. Surg. 164:643-54, 1966.
16. 15. Friedland, Gerald W., op cit..
17. Strictly speaking, the diaphragm is undefined in the hiatus. The PEL, that closes the potential opening, is the ligament of a muscle perpendicular to diaphragmatic muscle.
18. 16. Botha, G.S. Mueller, Radiological localization of the diaphragmatic hiatus. Lancet 1:662-4, 1960.
19. 17. O'Sullivan, G.C., DeMeester, T.R., Joelson, B.E., Interaction of lower esophageal sphincter pressure and length of sphincter in the abdomen as determinants of gastroesophageal competence. Am. J. Surg. 143:40-7, 1982.
20. 18. DeMeester, T.R., Pathophysiology of gastro-esophageal reflux. In: Disorders of the esophagus: advances and controversies. Eds. Watson, A. and Celestin, L.R., Pitman Publishing, Ltd., London, 1984.
21. 19. Pope, Charles E., II, Pathophysiology and diagnosis of reflux esophagitis. Progress in Gastroenterology, Gastroenterology 70:445-454, 1976.
22. 20. Dodds, W.J., NEJM 305: 1547-52, 1986.
23. Paradoxically, clinical manometrists - champions and custodians of the sphincter - who ignore the angle of His and valve of Guberoff in their daily work and in their publications, refer their therapeutic failures to surgeons for fundoplications!
24. 21.McCallum, R.W., Ippoliti, A.F., Cooney, C. et al., A controlled trial of metoclopramide in symptomatic gastroesophageal reflux. NEJM 296:354-7, 1977.
25. 22.Dent, J., Dodds, Wylie J., Friedman, R.H., et al., Mechanisms of gastroesophageal reflux in recumbent asymptomatic studies. J. Clin. Invest 65:256-67, 1980.
26. 23. Patricos, John, Martin, Christopher J. and Dent, John, Relationship of transient lower esophageal sphincter relaxation to postprandial gastroesophageal reflux and belching in dogs. Gastroenterology 90:545-51, 1986.
27. 24. Euler, Arthur R. and Byrne, William J., Twenty-four-hour esophageal intraluminal pH probe testing: a comparative analysis. Gastroenterology 80:957-61, 1981.
28. 25. Hillemeier, A. Craig, Grill, McCallum, Bruce B., et al., Esophageal and gastric motor abnormalities in gastroesophageal reflux during infancy. Gastroenterology 84:741-6., 1983.
29. 26. Hauser, R., Dodds, W.J., Patel, G.K., et al., Mechanism of gastroesophageal reflux in patients with reflux esophagitis. (Abstract) Gastroenterology 75:1153, 1979.
30. 27. Levin, Mark S., Gastroesophageal junction, In: Gastrointestinal Radiology, Eds, Gore, Richard M., Levin, Mark S. & Laufer, Igor, Eds., W.B. Saunders, Philadelphia, 1994.
31. 28. Behar, Jose, In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Curchill Livingstone, New York, 1982.
32. 29. Sweeting, J., Gastroesophageal reflux. Gastroenterology 85:477-8, 1985.
33. 30. Fournet, Jacques, Snape, William J. and Cohen, Sidney, The cholinergic component of lower esophageal sphincter pressure: a comparison of findings in the opossum and in the cat. In: Gastrointestinal Motility, Ed. Christensen, James, Raven Press, New York, 1980.
34. 31. Diamant, Nicholas E., Normal esophageal physiology. In:Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
35. 32. Dodds, Wylie J., Dent, J. and Hogan, W.J., Pregnancy and the lower esophageal sphincter. Gastroenterology 74:1334-35, 1978.
36. 33. Cohen, S. Motor disorders of the esophagus. New Eng. J. of Med. 301:184-92, 1979.
37. 34. Vantrappen, G., Jannsens, J. and Coremans, G., Gastroenterology 76:450-57, 1979.
38. 35. Ippoliti, Andrew F. and Varner, Albert A., Does denervation of the lower esophageal sphincter occur in diffuse esophageal spasm? In: Gastrointestinal Motility, Ed. Christensen, James, Raven Press, New York, 1980.
39. 36. Dent, J., Dodds, Wylie J., Hogan, W.J. and Arndorfer, R.C., Pressor effect of cholecystokinin-octapeptide on the opossum lower esophageal sphincter. In: Gastrointestinal Motility, Ed. Christensen, James, Raven Press, New York, 1980.
40. 37. Dent, John, What's new in the esophagus? Dig. Dis. Sci. 26:161-73, 1981.
41. 38. Edwards, M.H., Selective vagotomy of the canine esophagus - a model for the treatment of hiatal hernia. Thorax 31:185-9, 1976.
42. 39. Harrington, S.S., Dodds, W.J. and Mittal, R.K. Identification of longitudinal muscle activity in opossum lower esophageal sphincter. Am. J. Physiol. 261:G974-80, 1991.
43. 40. Goyal, R.K. and Rattan, S., Genesis of basal sphincter pressure: Effect of tetrodotoxin on lower esophageal sphincter pressure in opossum in vivo. Gastroenterology 71:62-7, 1976.
44. 41. Blank, E.L., Holloway, R.H., Dodds, Wylie J., et al., Neural contribution to LES pressure in conscious opossums. (Abstract) Gastroenterology 90:1315, 1986.
45. 42. Dodds, Wylie J., Stewart, E.T., Hogan, W.J., et al., Opening mechanism of the feline lower esophageal sphincter. (Abstract) Gastroenterology 64:718, 1973.
46. 43. Torrance, H. Bruce, Studies on the mechanism of gastro-esophageal regurgitation. J. Roy. Co. Surg. (of Edinberg) 4:54-62, 1957.
47. 44. Johnson, H. Daintree, Active and passive opening of the cardia in relation to the pathogenesis of hiatus hernia. Gut 7:392-401, 1966.
48. 45. Goldberg, Henry I. and Scheft, Douglas J., Esophageal and colon changes in myotonia dystrophica. Gastroenterology 63:134-9, 1972.
49. 46. Pierce, J.W., Creamer, B. and McDermott, V., Pharynx and esophagus in myotonia dystrophica. Gut 6:392-5, 1965.
50. 47. Hughes, D.T.D., Swan, J.C., Gleeson, J.A. and Lee, F.L., Abnormalities in swallowing associated with dystrophia myotonia. Brain 88:136-45, 1965.
51. 48. Vanhoutte, Jean J., Baghdassarian Gatewood, Olga M., Talbert, James L., Brooker, B.A. and Haller, J.Alex, Jr., Cinefluorographic and manometric evaluation of the motor function of the esophagus following segmental resection in newborn dogs. Radiology 86:718-722, 1966.
52. 49. Jannsens, J., The peristaltic mechanism of the esophagus. Acco, Lueven, 1978. Cited by Diamant, Nicholas E. In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
53. 50. Boyle, John T., Congenital disorders of the esophagus. In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
54. 51. Louhimo, Ilmo, Sulamaa, Matti and Suutarinen, Toivo, Postoperative intensive care of esophageal atresia patients. J. Pediatr. Surg. 5:633-40, 1970.
55. 52. Hands, Linda J. and Dudley, N.E., A comparison between gap-length and Waterson classification as guides to mortality and morbidity after surgery for esophageal atresia. J. Ped. Surg. 21:404-6, 1986.
56. 53. Vanhoutte, Jean J., Baghdassarian Gatewood, Olga M., Talbert, James L., Brooker, B.A. and Haller, J.Alex, Jr. Cinefluorographic and manometric evaluation of the motor function of the esophagus following segmental resection in newborn dogs. Radiology 86:718-722, 1966.
57. 54. Jannsens, J., The peristaltic mechanism of the esophagus. Acco, Lueven, 1978. Cited by Diamant, Nicholas E. In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
58. 55. Boyle, John T., In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
59. Perhaps it should. Rupture of the PEL and widening the hiatus could be expected to prevent this complication.
60. 56. Collis, J.L., Gastroplasty. Thoraxchirugie 11:57-63, 1963.
61. I have not found any reports that these iatrogenic Barrett esophaguses are more prone to malignancy.
62. 57. Skinner, David B., Reflux esophagitis. In: Bockus Gastroenterology, Fourth Edition, Vol. 2, Ed. Berk, J. Edward, W.B. Saunders Company, Philadelphia, 1985.
63. 58. Johnson, Lawrence F., Hiatal hernia influence on gastroesophageal reflux. In: Esophageal function in health and disease. Eds Castell, Donald O. and Johnson, Lawrence F, Elsevier Biomedical, New York, 1983.
64. 59. Edmunds, Vincent, Hiatus hernia: a clinical study of 200 cases. Quart. J. of Med. (New series) 26: 445-65, 1957.
65. 60.Wright, Richard A. and Hurwitz, Alfred L., Relationship of hiatal hernia to endoscopically proved reflux esophagitis. Dig. Dis. Sci. 24:311-3, 1979.
66. 61.Paterson, William and Kolyn, Donna M., Esophageal shortening induced by short-term intraluminal acid perfusion in the opossum: a cause for hiatus hernia? Gastroenterology 107:1736-40, 1994.
67. 62. DeMeester, T.R., Wernley, J.A., Bryant, J.A., et al., Clinical and in vitro analysis of gastroesophageal competence: a study of the principles of antireflex surgery. Am. J. Surg. 137: 139-47, 1979.
68. 63. Dodds, Wylie J., Hogan, Walter J., Helm, James F. and Dent, John, Pathogenesis of reflux esophagitis. Gastroenterology 81:376-94, 1981.
69. 64.Thomas, Fred B., Steinbaugh, Jan T., et al., Inhibitory effect of coffee on lower esophageal sphincter pressure. Gastroenterology 79:1262-6, 1980.
70. 65. Bickel, Martin and Kauffman, Gordon L., Jr., Gastric gel mucus thickness: effect of distention, 16,16-dimethyl prostaglandin E2, and carbenoxolone. Gastroenterology 80:770-5, 1981.
71. 66. Dougherty, R.W., Habel, R.E. and Bond, H.E., Esophageal innervation and the eructation reflex in sheep. Am. J. Vet. Research 70:115-128, 1958.
72. 67. Balfour, D.C. Jr., and Wharton, G.K., Oral procaine hydrochloride for the relief of cardiospasm. Gastroenterology 18:606, 1951.
73. 68. Henderson, Robert D. and Godden, John O., Motor disorders of the Esophagus Williams & Wilkins, Baltimore, 1976.
74. 69. Behar, Jose, In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
75. 70. Roth, James L.A., Bockus Gastroenterology, Vol 2, Fourth Edition, Ed. Berk, J. Edward, W.B. Saunders Company, Philadelphia, 1985.
76. 71. Vantrappen, G. and Janssens, J., Medical treatment of gastro-esophageal reflux. In: Disorders of the esophagus: advances and controversies. Eds. Watson, A. and Celestin, L.R., Pitman Publishing, Ltd., London, 1984.
77. 72. McCallum, Richard W., Recent advances in the medical therapy of gastroesophageal reflux. In: Esophageal Disorders, Eds. DeMeester, Tom R. and Skinner, David B., Raven Press, New York, 1985.
78. 73.Orlando, Roy C., Reflux esophagitis, I: Textbook of Gastroenterology, Yamanna, Tadataka, Ed. J. B. Lippencott, 1991.
79. 74. Pope, Charles E., II, Anti-reflux disorders, NEJM 331:656-60, 1994.
80. . Boisen, R,, Hamilton, J.W., Yamamoto, D., Wagner, J. And Reicheldorfer, M., The foam wedge is as effective as elevation of the head of the bed in reducing esophageal reflux. Abstract, Gastroenterology :1329, 1988.
81. 76. Johnson, Lawrence F. and DeMeester, T.R., Evaluation of elevation of the head of the bed, bethanechol, and antiacid foam tablets on gastrointestinal reflux. Dig. Dis. Sci. 26:673-80, 1981.
82. Assuming a 6 foot bed elevated on 1' bed blocks and an esophagus 22.8 cm in length, by similar triangles it works out that elevating the head of the bed raises the upper end of the esophagus 3.8 cm above the lower. This is .28 mm of Hg - half that for 6" blocks.
83. 77. Johnson, Lawrence F., Hiatal hernia influence on gastroesophageal reflux. In: Esophageal function in health and disease. Eds. Castell, Donald O. and Johnson, Lawrence F, Elsevier Biomedical, New York, 1983.
84. 78. Garretts, M., "Burning lips" associated with esophageal reflux. Lancet 3:1776-7, 1960.
85. This relief on cervical inteflexion may aid in the diferential diagnosis of angina vs. Pyrosis.
86. 79. Kinsbourne, M., Hiatus hernia with contortions of the neck. Lancet 1:1058-61, 1964.
87. 80. O'Donnell, J.J. and Howard, R.O.,Torticollis associated with hiatus hernia (Sandifer's syndrome). Amer. J. Opthamol. 71:1134-7, 1971.
88. 81. Sutcliffe, J., Torsion spasms and abnormal posture in children with hiatus hernia, Sandifer's syndrome. Progr. Pediat. Radiology 2:1190, 1969.
89. I suspect that the dorsiflexion provoked by eating is an effort to release the fundus from hiatal squeeze.
90. 82. Bray, Patrick F., Herbst, John J., Johnson, Dale G., et al., Childhood gastroesophageal reflux: neurologic and psychiatric syndromes mimicked. JAMA 237:1342-5, 1977.
91. 83. Williams, T.A., Boyle, J.T. and Altschuler, S.M., Opisthotonic posturing: a poor prognostic sign for outcome following Nissen fundoplication in children with mental motor retardation (MMR). Gastroenterology 90:1801, 1986.
92. 84. Pickhardt, O.C., Rafsky, H.A. and Gehiselin, F.H., Treatment of hiatus hernia in older persons. JAMA 142:310-14, 1950.
93. 85. Giuseffi, Vincent J., Grindley, John H. and Schmidt, Herbert H., Canine esophagitis following experimentally produced esophageal hiatus hernis. Proc. of the Mayo Clin. 29:14 399
94. 86. Mellow, Mark, Management of esophageal complications. In: Diseases of the esophagus. Eds. Cohen, Sidney and Soloway, Roger D., Churchill Livingstone, New York, 1982.
95. Some HH and antireflux operations, notably the Nissen procedure, destroy the PEL incidentally.
96. 87. Barrett, N.R., Hiatus hernia: a review of some controversial points. Brit. J. Surg. 42:231-43, 1954.
97. 88. Bombeck, C.T., Choice of operations for gastro-esophageal reflux. In: Disorders of the esophagus: advances and controversies. Eds. Watson, A. and Celestin, L.R., Pitman Publishing, Ltd., London, 1984.
98. 89. Schea, et al., op cit.
99. 90. Carlson, A. J., Boyd, T.E. and Pearcy, J.F., Studies on the visceral sensory nervous system. XIV. The reflex control of the cardia and lower esophagus in mammals. Arch. Int. Med. 30:409-33, 1923.
100. 91. Dent, John, Wylie J., Friedman, Robert H., et al., Mechanisms of gastroesophageal reflux in recumbent asymptomatic human subjects. J. Clin. Invest. 65:256-67, 1980.
101. 92. Longhi, W.J. and Jordan, P.H., Jr., Pressure relationships responsible for reflux in patients with hiatus hernia. SG&O 129:734-48, 1969.