Reflex control of the sphincter- the Cannon-Dougherty reflex
![]()
Normally we are quite unconscious of the nauseating odor and the highly disagreeable taste of the gastric contents, and for this pleasant security the closed cardia is responsible.
---- Walter B. Cannon(1) 1908.
Actually, in spite of many interesting theories we are still not certain why the trapeze artist is safe in the upside down position.
---- Richard Schatzki(2) 1965
These quotations, reflecting the importance of the subject on the one hand
and the unsatisfactory state of knowledge on the other, aptly epitomize the
"problem" of the lower esophageal sphincter.
The problem, as commonly formulated, requires an answer to two questions:(3)
Why does the closure mechanism yield to a pressure as low as 5 mm Hg from
above?
Why will intragastric pressures as high as 80 mm Hg fail to force it?(4)
Some of the solutions proposed are: a.) The angle of His, b. the valve of
Guberoff, c. the sling fibers of the right crus of the diaphragm, d. the pinchcock
at the diaphragm, e. the sphincter of Lerche,(5)
f. the bracket bundles,(6) g. the esophageal
vestibule as variously defined by Lushka,(7)
Arnold,(8) and Ingelfinger, et al.(9)
Lerche,(10) Hayward,(11)
and others, h. pouting of the gastric mucosa by the muscularis mucosae,(12)
i. differential pressure in the abdomen and thorax, j. the submerged segment
or "empty segment."(13) Singly or in combination,
a case can be made for many of these proposals.
The multiplicity of solutions should suggest that the basic problem has been
under defined. When two linear equations in three unknowns are specified, an
infinite number of solutions can be found. In the same way, the present problem
is so lacking in stringency that conjecturing solutions is too easy. These are
neither apt nor unique and fail when measured against the test of clinical and
radiological experience. It is not difficult to show that we must feed in more
conditions to be satisfied before we can test the various solutions.
Whole classes of solutions are ruled out by the circumstance that most instances
of reflux are temporary, intermittent and self limiting. The ingestion of raw
onions, radishes, martinis, smoked pork sausages, pizza and barbecued spareribs
can hardly alter the morphology! It is not obvious that any of the listed mechanisms
can account for this simple fact.
Similarly, in instances of infantile cardioesophageal reflux,(14)
when the condition is present, we can find no structural defect. When it clears
spontaneously, there is no alteration in architecture. It seems, therefore,
that purely morphological devices are excluded, i.e., it is improbable that
any of the listed mechanisms are so configured that they could explain the phenomenology.
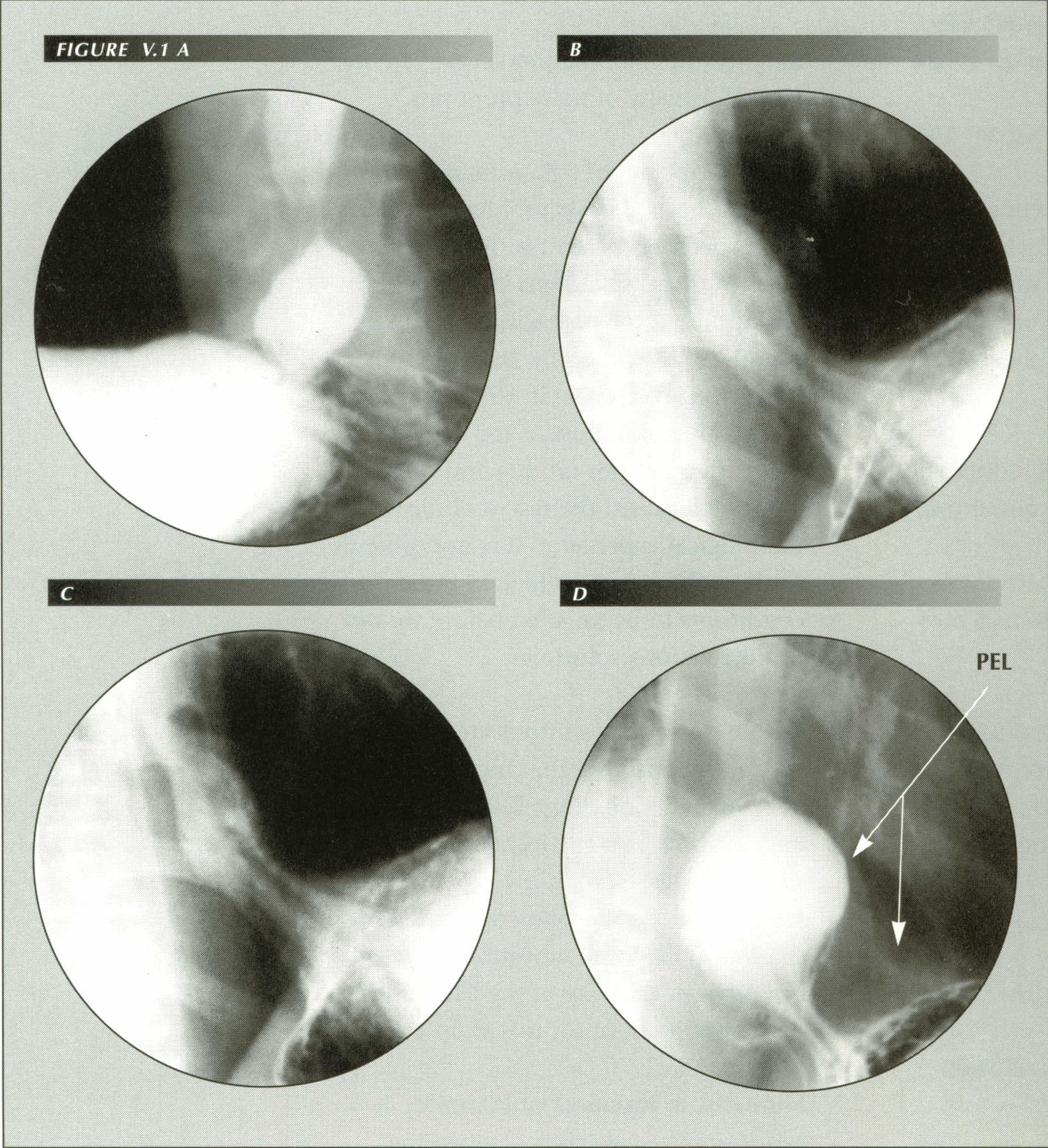
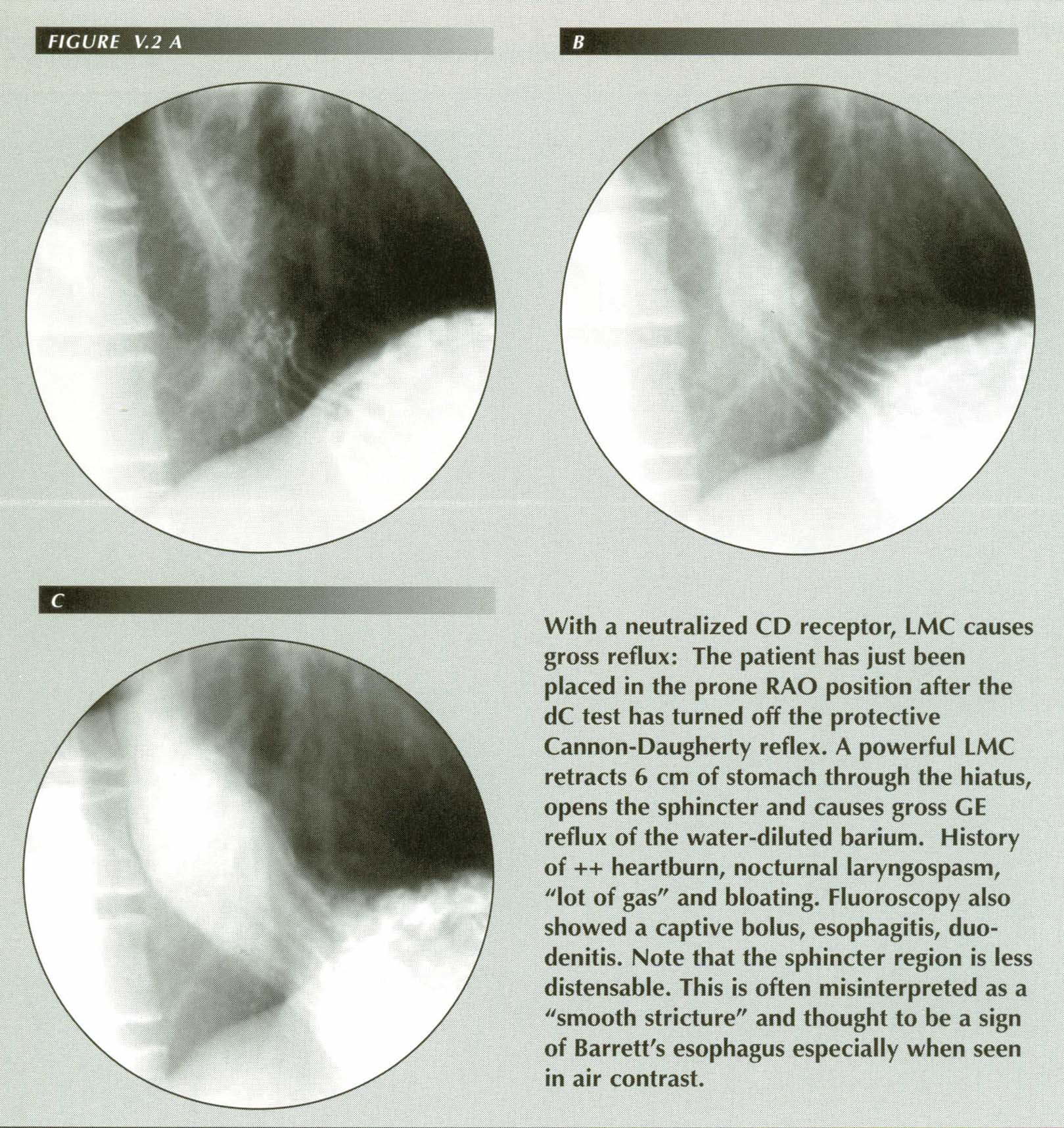
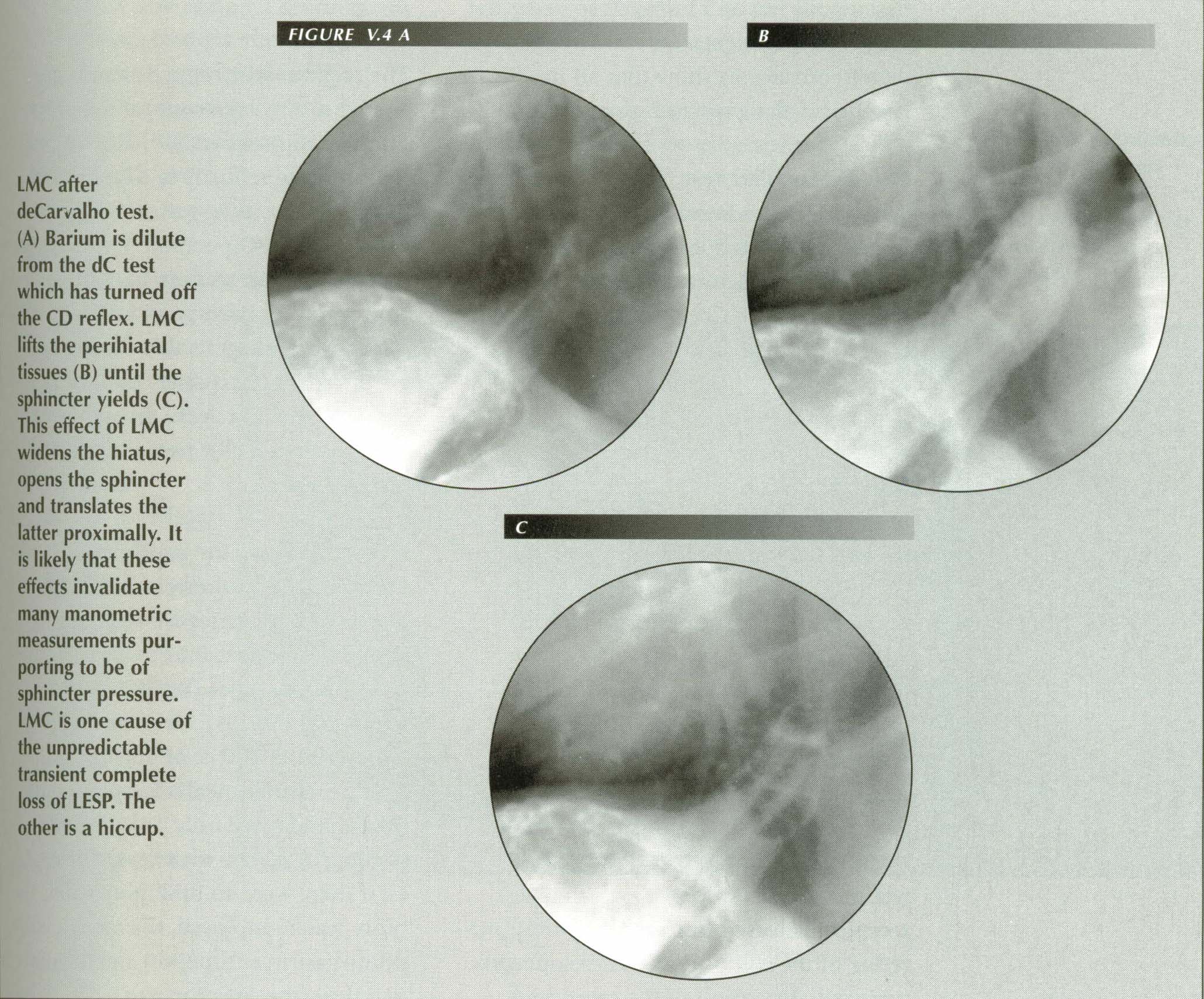
The Cannon-Dougherty reflex: If the posterior wall of the stomach is fluushed with water in the supine position (A) it may �turn of� the CD reflex that normally inhibits reflux. A hypertonic LMC then produces gross reflux of either air or gastric contents when the patient assumes the prone RAO position (B & C). When LMC occurs at this point one simply asks the patient if he has the gas or bloat symptom at that instant. The deCarvalho maneuver causes reflux in patients with a hypertonic LM because it neutralizes the CD inhibitory reflex. Compare the appearence of the gastric segment (a traction cone in (B) and (C) when a hiatal traction is produced by this method) with that (captive bolus) produced by the Valsalva test in the same patient (D). The faint outline of the PEL tent can be seen here.
![]()
Control must be precise
A more subtle, but equally persuasive, objection to most of the listed mechanisms
is the fact that, even were they workable, they would be too crude to account
for the perfection and nicety of control that is a matter of universal experience.
We can observe in ourselves and in patients that, although belching is common,
the eructation of acid with the gas is uncommon. The sphincter mechanism operates
as though it were a separatory funnel (in reverse) that permitted the flow of
gas but not of gastric fluid contents. Observed with a fluoroscope in the standing
patient, the air-fluid level in the stomach rises rapidly when the sphincter
opens to permit the release of gas. Yet it closes with great precision just
in time to prevent even a drop of fluid entering the esophagus.
Moreover, a mass of clinical lore concerning belching, burping (of infants),
esophageal speech, vomiting and so on, some of which will be detailed later,
cannot be explained by any purely morphologic mechanism proposed to date. These
phenomena are so intricate and so exactly executed that one simply has to take
as a starting point this postulate: There is a valve-equivalent mechanism
between esophagus and stomach that, under reflex control, is open when it should
be open and closed when it should be closed.
Writing about 1952, Delmas and Terracol(15)
in describing the lower esophagus state unequivocally, "It should be stressed,
however, that there is no muscular structure in this region, whether it be in
the diaphragm itself or in the tenuous fibers of Juvera and Rouget, which can
play the role of a sphincter."
Since then, modern physiologists(16),(17)
maintain that there is a zone of sustained high pressure in a short segment
of the distal esophagus that they believe is the sphincter. Although the sphincter
they believed they were recording was, as we have seen, illusory, there is a
genuine specialized ring of circular which provides this function.
The true sphincter obviously fulfills the function of preventing reflux of gastric contents. It can be forced with difficulty from below, yet mere gravity easily opens it from above. Just as obviously, the sphincter has no morphologic characteristics that would make it a 1-way valve. That such a simple structure can meet the demands upon it is due to the sophisticated reflex system that controls it.(18) An element of this system that can be traced in part to the work of W.B.Cannon but more particularly to the admirable experiments of R.W. Dougherty is the subject of this chapter.
![]()
Cannon's experiments
In 1903, Cannon,(19) working with cats, found
that when 180-220 cc of a bland solution of potato starch and bismuth subnitrate
was introduced into the stomach, it would reflux from stomach to esophagus,
be milked back into the stomach by a peristaltic wave and reflux again, repeatedly
in a regular back and forth pattern.
If the starch-bismuth preparation was then brought to the normal pH for carnivores
(.5%), one final reflux occurred and the back and forth motion ceased. Five
years later, he confirmed these fluoroscopic observations on the unanesthetized
animal by pressure measurements in the esophagus and gastric fundus of the anesthetized
cat.
Section of the splanchnic nerves did not affect the reflex closure. Section
of the vagus nerves five and seven days before the experiment and pithing the
animal to the brachial region practically eliminated the reflex, but after removing
the acid solution from the stomach and immediately reinjecting it, the pressure
required to force the sphincter from below increased from 19 cm of water on
the first try to 53 cm of water on the forth repetition. As he had eliminated
every extrinsic pathway that could be involved in reflex closure, Cannon had
to conclude that he was dealing with a locally acting "myogenic" reflex.(20)
Sphincter control in ruminents
After a lapse of two generations, R.W. Dougherty(21),(22),(23),(24),(25)
rediscovered the reflex closure of the cardia and, in a beautiful series of
experiments, added greatly to our understanding of the mechanism. Dougherty,
a veterinary physiologist, did the bulk of his work with ruminants, particularly
sheep, because of a peculiarity of this class of animal.
A ruminant can derive nourishment from low quality roughages because of a
huge forestomach, the rumen, which serves as a fermentation tank in which bacterial
decomposition of forage takes place. The nutrients thus released and modified,
and the bacteria themselves, are then further digested and absorbed in a fashion
comparable to the process in man.
Enormous quantities of gas evolve in this bacterial digestion. Hungate et
al. calculated that 1.2 liters of gas formed per minute in the
rumen and reticulum of a 1000 pound bovine animal. If this gas cannot be eliminated
properly, largely by eructation, the animal dies very quickly when the distended
rumen forces the diaphragm cephalad and embarrasses respiration. Consequently,
the ability to eructate gas, which in man would be but a minor annoyance, is
a fatal malfunction in the ruminant. This inhibition of gas release from the
reticulo-rumen is known as "bloat." According to some estimates, it is responsible
for an annual economic loss of $100,000,000 to cattle raisers.
Dougherty, Habel and Bond, working with decerebrate sheep, found that eructation
was inhibited if the area around the cardia were covered with water, ingesta,
foam or mineral oil. Eructation was also completely inhibited with the animal
on its back even if the intrarumenal pressure were raised to as much as 120
mm Hg by injection of carbon dioxide gas into a rumen fistula.
Although the cardiac sphincter could resist this high pressure, nevertheless, if the rumen were emptied of fluids so that it contained only gas, the animal eructated equally well in the supine position as it did in the prone. One hundred cc of water in the rumen of a small sheep would completely inhibit eructation in dorsal recumbency. When the water was removed and 100 ml of 1% butyn sulphate solution substituted, gas and fluid were eructated when the rumen was insufflated.
![]()
In later experiments employing cine-radiography, it was shown that the reticulum
contracted in such a way as to empty itself of ingesta. In these remarkable
films,(26) a fold can be seen rising out of
the floor of the cephalad portion of the reticulum. The fold then becomes more
prominent and moves caudally pushing ingesta in front of it away from the mouth
of the esophagus and acting as a small dam to keep it away.
In this way, the reticulum empties itself of gas by erecting a barrier over
which gas can flow out the esophageal orifice while the fluid content of the
rumen is held clear of the esophageal mouth thus preventing contact of ingesta
from the region so that reflex inhibition of eructation will not occur. The
speed and forcefulness of this activity leave no doubt that it is purposeful
and that the purpose is to clear the way for eructation.
Neurologic control of the sphincter
Stevens and Seller(28) showed that eructation
could be inhibited by procaine hydrochloride block of the dorsal vagal trunk
on the one hand and promoted by stimulation of the same nerve trunk.(29)
The conclusion of the Dougherty group, therefore, is that there are receptors
in the stomach epithelium immediately next to the mouth of the esophagus
that, when stimulated by the presence of ingesta, reflexly inhibit opening of
the lower esophageal sphincter. The experimental results also would show that
the reflex is mediated through the vagus and, presumably, higher centers. This
conclusion corrects the earlier view of Cannon who believed he was dealing with
a local "myogenic" reflex.
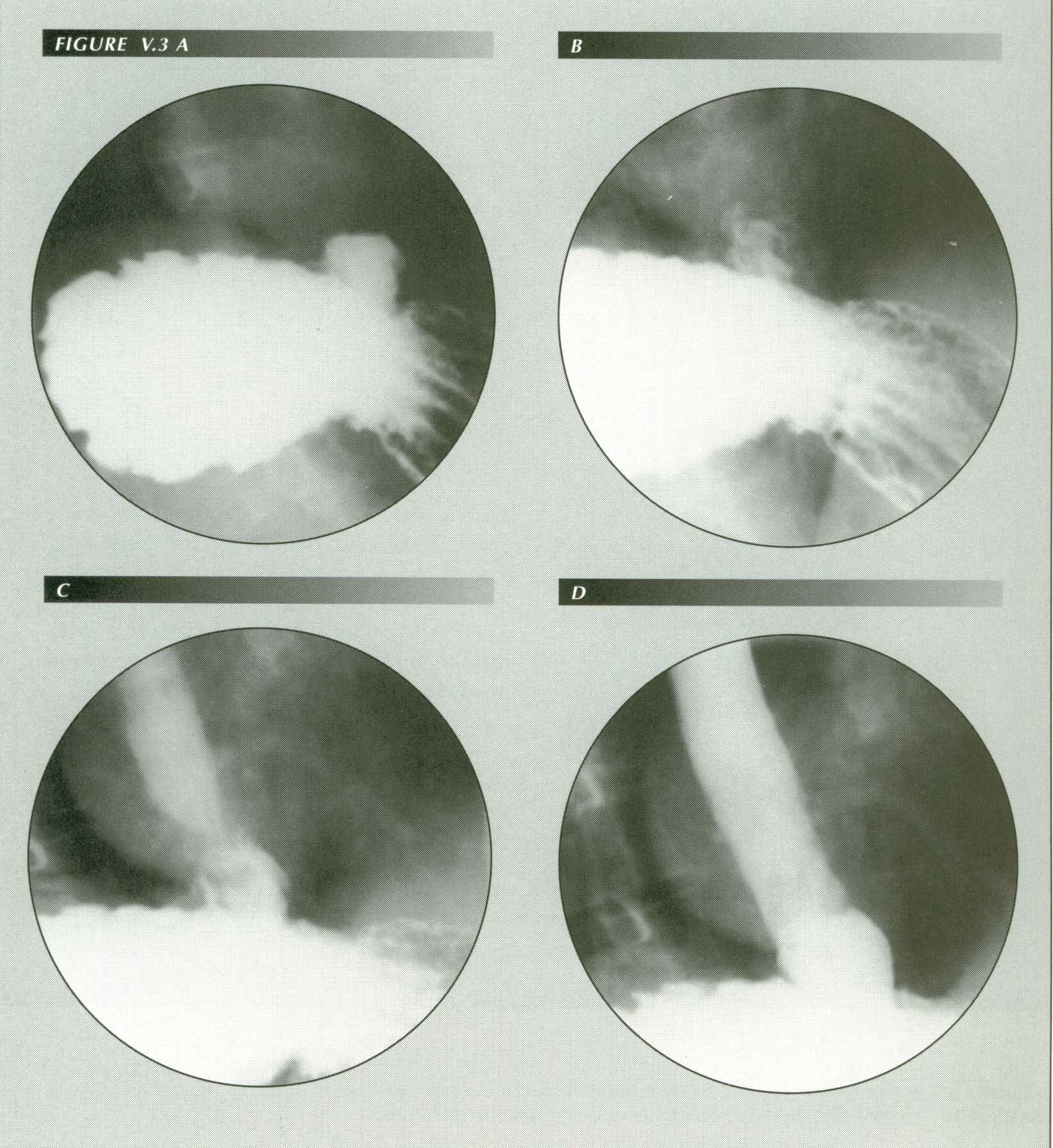
The de Carvalho test: Frame(A) shows barium in a short tube of stomach above the diaphragm. In frame (B), it is diluted by water being swallowed by the patient in the RPO position (supine, right side down). The sphincter is still closed, however. In frame (C) refluxing barium is diluted by water in the esophagus as the CD receptor is flushed. By frame (D) the entire esophagus is flooded with refluxed barium. This is the time to ask the patient a.) whether he can feel something coming back up and b.) whether it reproduces his symptom in all but degree. Both cats (Cannon) and ruminants (Dougherty) have a sensory area near the mouth of the esophagus that inhibits LM contraction when stimulated by ingesta. The de Carvalho maneuver, as shown here, washes this area free of ingesta allowing reflux to occur in patients with high LM tension.
![]()
Human applications
Several objections that must be overcome before we can confidently apply these results to man:
1.) Dougherty was dealing with the highly specialized digestive tract of the
ruminant. The multi compartment stomach, the largely striated muscle of the
esophagus, the fact that there are not separate longitudinal and circular muscle
layers (there are two oblique layers instead) all suggest caution.
2.) Although Cannon's experimental animal, the cat, is one from which experimental
results can usually be extrapolated to man, the reflex - at least as he interpreted
it - seems inapplicable on several counts:
a.) Rhythmic back and forth motion of fluid between the stomach and esophagus
is not normally observed in man.
b.) An unphysiologic amount of fluid was given to the intubated animals in
the fluoroscopic studies (180-200 cc of fluid is the entire normal daily intake
of a large cat.)
c.) In interpreting his experiments, Cannon seems to have neglected the possibility that there might be a reflex that opened the sphincter or decreased sphincter tone.
The response to these difficulties is to turn our attention directly to the question of whether an inhibitory reflex, especially of the type showed by Dougherty, exists in man. The reflex can be studied in routine radiologic examinations of the upper GI tract and the highly sophisticated equipment now in common use compensates for the fact that we are not as a rule able to perform surgical experiments. Several lines of evidence converge to show that an inhibitory reflex is also present in humans
![]()
The de Carvalho test
When water is administered to a patient in the right posterior oblique (supine)
position, in some cases, cardioesophageal reflux will occur. Crummy(30)
found this to be true in 10.3% of 650 consecutive cases. Linsman(31)
encountered an incidence of 40.5% of 1000 cases. Although there seems to be
good correlation between a positive dC test and a history of pyrosis, the question
"What does the dC test?" is still an open one.
Yet Cannon's experiments provide an answer. When he administered a large quantity
of starch-bismuth solution to cats and observed rhythmic reflux, he was basically
performing a de Carvalho test. That is, the stomach was flooded with water and
any acid present was washed away or diluted to the point where it could no longer
activate the receptor. Released from reflex inhibition, reflux of the solution
into the esophagus occurred, distention of the esophagus reflexly caused peristalsis,
and so on. The more prolonged the experiment, the less frequent were the episodes
of reflux suggesting that accumulating acid /pepsin reactivated the reflex.
If the CD reflex is present in man, then the deCarvalho test can be explained
in exactly the same way: the barium meal dilutes any acid/pepsin already in
the stomach and the water administered in the RPO position washes over the CD
receptor flushing it further. In this way, Cannon's experiment is reproduced.
Gastric contents reflux and are milked back into the stomach by peristalsis.
The angle at which the patient is positioned is often quite critical corroborating
this interpretation. The best way to demonstrate reflux is to have the patient
drink rapidly, as he turns from supine toward the RPO position. Reflux starts
at a definite point and usually stops when this point has been passed. This
position dependence suggests that the stream of water must be accurately directed
at the receptor area to release the sphincter. It also provides a clue to the
location of the receptor.
If one compares the parallel studies of Linsman and Crummy, we find that,
although both series are qualitatively similar, reflux was four times as frequent
in Linsman's series (40.5%) as in Crummy's (10.3%). Linsman had the patient
drink 200 cc of water after the routine barium meal. Crummy, on the other hand,
used only 15-30 cc. These results are exactly what would be expected if there
were an inhibitory reflex: the more water employed, the more it will dilute
gastric acid/pepsin and the more it will flush the receptor area. Consequently,
the more patients in whom the CD receptor will be turned off allowing reflux.
A Chi square test for significance shows a positive association between reflux
symptoms and a positive deCarvalho test (p < .005). It shows that, once the
inhibitory reflex is turned off, whatever is operating to cause sphincter release(32)
will be uninhibited. The significance of the difference (p < .001) between
the frequency of reflux in the otherwise parallel series of Crummy (10.3%) and
Linsman (40.5%) also supports the above interpretation.
In these patients, as with the sheep in Dougherty's experiments, the receptor
must be on the posterior wall of the stomach - the area washed by the stream
of water entering the stomach in the deCarvalho maneuver.
Magenblase

Freed of the inhibitory reflex, the LM contracts and causes reflux. Note proximal displacement of sphincter.
![]()
Other evidence of a CD reflex
There are some pyrosis patients in whom the sphincter remains open for periods
of 20 seconds or more. If during this time, they are tilted so that the gastric
fluid approaches the mouth of the esophagus, the sphincter will close.
Even more striking is the occasional patient with myotonic dystrophy. In this
condition, with esophageal involvement, the sphincter is always widely
patent. As a result, the patient swallows air to keep gastric contents out of
the esophagus. The air column extends from the cervical esophagus to the gastric
sinus. Even in such a patient, the sphincter will close, however ineffectually,
when gastric contents are maneuvered into the proximity of the mouth of the
esophagus.
If acid/pepsin is required to activate the receptor, it would be expected
that removal of the acid secreting portion of the stomach would cause a failure
of sphincter inhibition and consequently reflux. This complication has been
described by Lataste and Gonthier.(33) Again,
if there is a loss of gastric acid production from atrophic gastritis there
is increased reflux. In this condition the pH may be > 5 instead of the normal
< 3.(34)
Turning to evidence that is perhaps less "scientific" but nevertheless useful
as a check on the conclusions, we recall that mothers burping infants invariably
place them in exactly the position that places air rather than gastric fluid
in contact with a receptor area on the posterior wall of the fundus. To do otherwise
would bathe the receptor area with gastric fluid and activate the inhibitory
reflex.
Most people I have questioned have noted subjectively that they automatically
lean forward when a premonitory sensation of subxiphoid tension signals an impending
eructation. This is most obvious when drinking a carbonated beverage while seated
in a reclining chair. One is also conscious of this forward inclination of the
body when driving a car as the shoulder strap of the seat belt interferes with
the motion and brings it to attention.
Physicians and nurses also note that when bed patients vomit or belch they
struggle to turn toward the prone position thus freeing the CD receptor from
contact with gastric contents and releasing the sphincter-opening mechanism.
The sensation of "gas," paradoxically, is relieved by the ingestion of bicarbonate of soda although the resulting generation of CO2 when it contacts gastric acid should, one would think, aggravate it by increasing the amount of gas in the stomach. The immediate effect of ingestion of sodium bicarbonate is to produce an average of 4 cc (!) of gas in the first minute after ingestion. The reason is that, although the reaction is instantaneous, the gas produced remains in solution.(35)(36)
Neutralization of acid in contact with the CD receptor, however, can explain the relief as this permits sphincter release permitting eructation.
![]()
SUMMARY
The weight of the evidence derived from these diverse phenomena supports the
existence in humans of a reflex essentially identical with that reported by
Cannon in cats and elucidated in great detail by Dougherty and coworkers in
ruminants. This reflex has a gastric receptor, the physiologic sphincter of
the lower esophagus as an effector and a vagal reflex arc. There is evidence
that the receptor is on the posterior wall of the fundus.
This reflex explains the phenomena encountered in the deCarvalho "water siphonage
test" and the ease of eructating gas in contrast to the difficulty of disgorging
fluid gastric contents. It accounts for the "pleasant security" of Cannon and
the safety of Schatzki's trapeze artiste.
To be sure, this important reflex is not the only one affecting the sphincter. For example, it has been shown(37),(38),(39) that acid stimulation of the esophageal mucosa causes increased basal production of HCl in the stomach. This seemingly paradoxical vicious circle may actually serve the organism by feeding back a signal that will stimulate the CD receptor and thus close the sphincter.
These experiments do not, however, reveal how inhibition is accomplished. We must recall that the sphincter is normally closed. Therefore, one cannot simply assume that there is reflex tightening of the sphincter. Instead one must look for the mechanism that opens the sphincter, because that is what is actually being inhibited. In a subsequent chapter, I will assemble the evidence for this mechanism.
![]()
References
Last Updated July 26, 2007 by David PJ Stiennon
1. . Cannon, Walter B. Acid closure of the cardia. Am. J. Physiol. 23: 105-14, 1908.
2. . Schatzki, Richard, Esophagus: progress and problems. Am. J. Roentgenol. Rad. Therapy & Nuclear Med. 94: 523-40, 1965.
3. . Dornhurst, A.C., Harrison, K., and Pierce, J.M., Observations on the normal esophagus and cardia. Lancet 1: 695-98, 1954.
4. . Dornhurst, A.C., et al., op cit.
5. . Lerche, W., The esophagus and pharynx in action. Charles C. Thomas, Springfield, Illinois, 1950.
6. . Ziano, C., Poppel, M.H., Jacobson, H.G., Lepow, H. and Osturk, C.G., Lower esophageal vestibular complex: anatomic roentgen study. AJR 84:1044-54, 1960.
7. . Sycamore, L.K., Radiologic diagnosis of hiatus hernia. Gastroenterology, 31:169-89, 1956.
8. . Cited by Sycamore, Idem.
9. .Ingelfinger, F.J., Kraemer, P., and Sanchez, G.C., Gastroesophageal vestibule, its normal function and its role in cardiospasm and gastroesophageal reflux. Am. J. M. Sc. 222:417-25, 1954.
10. .Ingelfinger, et al., op cit.
11. . Hayward, J., The lower end of the esophagus. Thorax 16: 36-41, 1960.
12. . Barrett, R.N. Hiatus hernia, a review of some controversial points. Brit. J. of Surg. 42:231-244, 1954.
13. 13. Wolf, B.S., Roentgen features of the normal and herniated esophago-gastric junction. Problems in terminology. Am. J. Dig. Dis. 5:751-69, 1960.
14. . Neuhauser, E.D.B., and Berenberg, W., Cardio-esophageal relaxation as a cause of vomiting in infants. Radiology 48:480-83, 1947.
15. . Delmas, J., and Terracol, J. In: Gastroenterology, Vol 1, Bockus, H.L.,W.B.Saunders Company, Philadelphia, 1963.
16. 16. Code, C.F., Creamer, B, and Schlegel, J.R., An atlas of esophageal motility in health and disease, Charles C. Thomas, Springfield, Illinois, 1958.
17. 17. Ingelfinger, R.J., Esophageal motility. Physiol. Rev. 38:533-84, 1958.
18. It has been estimated that there are as many neurons in the gut as there are in the spinal cord. These include primary afferent, integrative and motor neurons.
19. 18. Cannon, W.B., Acid closure of the cardia. Am.J. Physiol. 23:105-114, 1903.
20. Chemical denervation with tetrodotoxin (TTX) also leaves baseline sphincter tone intact.
21. 19. Dougherty, R.W., and Meredith, C.D., Cinefluorographic studies of the ruminant stomach and of eructation. Am. J. Vet. Res. 16:96-100, 1955.
22. 20. Dougherty, R.W. and Habel, R.E. and Bond, H.E., Esophageal innervation and the eructation reflex in sheep. Am. J. Vet. Res. 19:115-28, 1958.
23. 21. Dougherty, R.W., The physiology of eructation in ruminants. In Digestive physiology and nutrition in the ruminant, Ed. Lesi, D., Butterworth & Company, London, 1960. (Proceedings of the University of Nottingham seventh Easter school in agricultural science, 1960)
24. 22. Dougherty, R.W., Bloat in ruminants, In: Forages, Eds. Hughes, H.D., Heath, M.W. and Metcalf, D.S., The Iowa State University Press, 2nd Edition, 1962.
25. 23. Hungate, R.E., Fletcher, D.W., Dougherty, R.W., and Barrentine, B.F., Microbial activity in the bovine rumen: its measurement and relation to bloat. Applied Microbiology 3:161-73, cited by Dougherty in Forages reference.
26. Which Dr. Dougherty very kindly allowed me to copy.
27. 24. Hill, K.J., Nervous structures in the reticulo-rumenal epithelium of the lamb and kid. Quart. J. of Exp. Physiol. 44:222-28, 1959.
28. 25. Stephens, C.E. and Sellers, A.F., Physiological studies of the vagal nerve supply to the bovine stomach. III. Procaine effects on the dorsal vagal trunk. Am. J. Vet. Res. 17:588-93, 1956.
29. These effects can equally well be cited as evidence that there is a sphincter opening reflex which travels along the same pathways.
30. 26. Crummy, Andrew B., The water test in the evaluation of gastro-esophageal reflux. Radiology 87:501-4, 1966.
31. 27. Linsman, J.F., Gastroesophageal reflux elicited while drinking water (water siphonage test); its clinical correlation with pyrosis. Amer. J. of Roentgenol. Rad. Ther. & Nuclear Med.
94: 325-332, 1965.
32. It will be shown that this is LM tension.
33. 28. Lataste, J. and Gonthier, F., Les reflux oesophagiens apre gastrectomies distales. La Presse Medicale 75:1025-28, 1967.
34. 29. Earlam, op cit.
35. The Editor of the National Geographic, who suffered a ruptured stomach after ingestion of 1 teaspoon of soda bicarbonate, attempted to place the blame on the soda and sued Arm & Hammer Corporation. His lawyers found " . . . about 18 cases of stomach rupture associated with baking soda . . . " in the world medical literature but " . . . an independent study commissioned by the company . . . concluded that baking soda produced too little carbon dioxide in a short period to be a likely cause . . . " The jury declined to award damages.
36. 30. Fordtran, John S., Morawski, Stephan G., Santa Ana, Carol A. and Rector, Floyd D., Gas production after reaction of sodium bicarbonate and hydrochloric acid. Gastroenterology 87: 1014-21, 1984.
37. 31. Giles, G.R., Clark, C.G. and Buchan, R., Effect of esophageal perfusion with acid on basal gastric secretion. Gut 9:52-6, 1968.
38. 32. Collis, J. Liegh, The causes of the variable response to gastric reflux in hiatus hernia. Royal Col. of Surg. of Edinb. : 77-87, 1969.
39. 33. Alwin, J.A., Thorax 8:38, 1953. Cited by Collis.